Download
1 / 42
420 likes | 540 Views
Determinants of Myocardial Performance. Afterload - The resistance to flow. The size of the arterioles. Which patient has the highest afterload? (A) 120/80 (B) 220/80. Determinants of Myocardial Performance. Which patient has the highest afterload? (A) 120/80

E N D
Determinants of Myocardial Performance • Afterload - The resistance to flow. The size of the arterioles. • Which patient has the highest afterload? (A) 120/80 (B) 220/80
Determinants of Myocardial Performance • Which patient has the highest afterload? (A) 120/80 (B) 220/80 • (A) - EF 15% Pulmonary Edema cool skin • (B) - 15 y/o 18 min. of Bruce ETT
Determinants of Myocardial Performance • Which patient has the highest afterload? (A) 120/80 • (A) - EF 15% Pulmonary Edema cool skin cardiac out put is 3 l/min
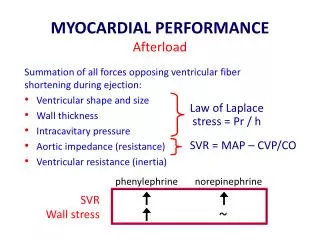
Determinants of Myocardial Performance • AfterloadSVR = (Mean BP - CVP) * 80/CO • (A) - EF 15% Pulmonary Edema cool skin SVR = (93.3-10)*80/3 = 2222 • (B) - 15 y/o 18 min. of Bruce ETT SVR = (126.6-5)*80/20 =486
Determinants of Myocardial Performance • AfterloadSVR = (Mean BP - CVP) * 80/CO or Cardiac output = Mean BP*80/SVR Cardiac output in patients even with low blood pressure can be increased by lowering SVR Do not be afraid of gradually increasing ACEI Cardiac output should be high More medication is therefore good
Determinants of Myocardial Performance • Afterload - The resistance to flow • How do we decrease Afterload? Vasodilators Nitroprusside, Natrecor ACEI / ARB Hydralazine/Nitrates MechanicalBalloon Pump
Determinants of Myocardial Performance • Contractility Inotropy • The speed and shortening capacity of the myocardium
Determinants of Myocardial Performance • Contractility Inotropy • The speed and shortening capacity of the myocardium • How is contractility increased? • The only oral agent - Digoxin • IV - Beta Agonist - Epinephrine Dopamine Levophed Dobtuamine Isuprel - Phosphodiesterase Inhibitors - Amrinone Milrinone Viagra
Determinants of Myocardial Performance • Compliance Lusitropy - the ability of the heart to fill Pericardium
Determinants of Myocardial Performance • Compliance Lusitropy - the ability of the heart to fill LVH, infiltrative excess calcium
Diastolic Heart Failure 25 15 5 vol1 vol2
Determinants of Myocardial Performance Compliance Lusitropy - the ability of the heart to fill. • How can we improve Compliance? • Natrecor • Spironolactone • Ranolazine
Physical Exam • Preload JVD (R), S3 and/or rales (L) • Afterload Carotid pulse (L), systolic pulmonary artery tap (R) • Contractility PMI (L) • ComplianceS4 (R) These simple physical findings should completely describe the heart’s performance and determines the medications that help
Equation of Life CO X Hgb = O2 consumption / AV O2 difference • Cardiac output X Hemoglobin • The lower the blood count the higher the cardiac output • You can compensate for lower cardiac output by having a higher blood counts Anemia (low blood count) is associated with CHF
How do CHF Patients suffer as they die? • Wide range of symptoms, which were frequently distressing and often lasted greater than 6 months Pain was most common in 50% Dyspnea was second most common Low mood, anxiety urinary incontinence Living and dying with heart failure: the role of palliative care Gibbs, McCoy,Gibbs,Rogers, Addington-Hall Heart 2002;88(supplII);ii36-ii39
How do your CHF Patients die? • Ventricular tachycardia/fibrillation • Pulseless electrical activity after a defibrillator shock • Pump failure low output • Sepsis from GI track due to bowel ischemia • Congestion and respiratory failure • Infection from skin breakdown • Liver or kidney failure • Inadequate reserve to meet extra demand
CHF patients can choose their mode of death • 28% of deaths can be avoided by defibrillator therapy • The mode of death changes to PEA, low out put, congestion or organ failure, failure to meet increase demands • Defibrillators are not for everyone
Strongest indicators of in-hospital death Fonarow GC et al.JAMA 2005; 293:572-580.
Heart Failure in Women: Overview • Affects older women disproportionately • Risk factors include hypertension, diabetes, obesity • More likely to have heart failure with preserved systolic function • Better prognosis than in men • Worrisome evidence of lesser responsiveness to ACE inhibitors; similar responsiveness to b-blockers
Heart Failure in African Americans: Overview • Affects 3% of the African American population • Atypical natural history • Unique epidemiology • Lower incidence of associated epicardial coronary artery disease • More likely to be associated with a historyof hypertension • Worrisome prognosis • Higher rate of hospitalization • Likely to have similar mortality risk • Question of altered responses to medical therapy Yancy CW. J Card Fail. 2000;6:183–186.
Heart Failure in African Americans: Etiology • Unique natural history • Occurs at an earlier age • Associated with more advanced left ventricular dysfunction at time of diagnosis • Worse clinical class at time of diagnosis • Higher incidence of left ventricular hypertrophy, especially concentric hypertrophy • Lack of definitive relationship between psychosocial factors and onset of disease Yancy CW. J Card Fail. 2000;6:183–186.
Etiology of Heart Failure inAfrican Americans Patients With Coronary Artery Disease-Based HF 80 60 40 Percent 20 0 V-HeFT I V-HeFT II SOLVD US Carv MERIT-HF BEST Patients With Hypertension-Based HF 80 60 Percent 40 20 0 V-HeFT I V-HeFT II SOLVD US Carv BEST MERIT-HF % AA % non-AA The BEST Investigators. N Engl J Med. 2001;344:1659–1657; Packer M et al. N Engl J Med. 1996;334:1349–1355; MERIT-HF Study Group. Lancet. 1999;353:2001–2007; Cohn JN et al. N Engl J Med. 1986;314:1547–1552;Cohn JN et al. N Engl J Med. 1991;325:303–310; The SOLVD Investigators. N Engl J Med. 1991;325:293–302.
Pearls • Dizziness - reduce, D/C diuretics • Look for exacerbation reasons ( atrial arrhythmia, anemia, non-compliance) • CHF drives salt and fluid cravings - constantly remind your patients -daily weight • avoid NSAID’s (Advil Motrin) • erythropoiten is very good • Add Hydralazine/nitrates for failures consider ARB addition to ACE
Patient Flow • Hand off between hospital and out patient therapy • Titrate medications & with compliance D/C Diuretic • Educate in salt, potassium, fluid balance, and weight • Not getting better Bi – V Defibrillator • equation of life • Monitor for non compliance – social/economic issue • Hydralazine /nitrate or ARB • Consider Geometric solutions & control of ectopy • Prometheus EECP and stem Cells Co Q 10 • Look for new endocrine failures for hypotension • Statins Statins Statins • Back off - Hospice or Transplant
Patient seems well with persistently elevated BNP BNP Brain Naturetic Peptide - a Heart Hormone < 120 heart is happy Can be compensated when elevated Know your number
Last Pearl • Good is Better • The Enemy of Good is Better • i.e. -Watermelon Syncope
Stem Cells the Future • Regenerative Medicine • Control of Inflammation • Electrical Remodeling The future is now Exercise increases stem cells
Summary • Heart failure is expensive and causes suffering • Heart Failure can improve with good life quality • Patients need to have good nutrition and avoid excess salt, fluids, calories • Patients need to take medications as prescribed and understand their purpose • Exercise 1 hour per day • Help your Doctors Nurses Dieticians with your complaints and work together for a solution • If these simple instructions are followed expensive operations might be avoided