Download
1 / 41
500 likes | 1.14k Views
Insulin Resistance in Children. Kellie Bryant. Introduction. Type 2 diabetes once considered a disease of adults has increased dramatically since 1980 in children. One third of all children less than 18 years of age diagnosed with diabetes have type 2.

E N D
Insulin Resistance in Children Kellie Bryant
Introduction • Type 2 diabetes once considered a disease of adults has increased dramatically since 1980 in children. • One third of all children less than 18 years of age diagnosed with diabetes have type 2. • The incidence of type 2 diabetes have paralleled the prevalence of obesity.
Type 2 diabetes in children is most commonly diagnosed at puberty. • One of the major characteristics of type 2 diabetes is insulin resistance which is considered the hallmark of type 2 dm.
Physiologic Effects of Insulin • Insulin is a hormone produced in the beta cells of the pancreas. • Insulin is formed from proinsulin • When the pancreas is stimulated by elevated blood glucose proinsulin is broken a part leaving insulin and C-peptide. • Both are secreted and enter the blood stream in equimolar amounts. • Normal insulin—0.5-0.7 units/kg of body weight per day.
Insulin’s Effects on Body Tissues • Stimulates entry of amino acids into cells—enhances protein synthesis • Enhances fat storage and prevents the mobilization of fat for energy • Stimulates the entry of glucose into cells to use as an energy source • Promotes the storage of glucose as glycogen in muscle and liver cells • Inhibits production of glucose from liver or muscle glycogen • Inhibits the formation of glucose from non-carbohydrates
Since insulin and C-peptide are jointly secreted, either can be used to monitor endogenous insulin production. • Normal values for fasting serum insulin and C-peptide are 0-30 µIU/ml
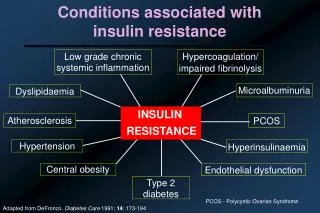
Characteristics of Insulin Resistance • Metabolic state characterized by fasting and or postprandial hyperinsulinemia • Reduced hepatic and skeletal muscle insulin sensitivity is compensated for by increased pancreatic insulin secretion to maintain normal blood glucose, which overtime contributes to the development of postprandial hypergycemia.
Therefore, insulin resistance is most familiarly associated with type 2 diabetes and seen in two prediabetic states—impaired fasting glucose and impaired glucose tolerance (most recently referred to as pre-diabetes.
Insulin resistance is also associated with hypertension, dyslipidemia and coronary heart disease. • It is speculated that hyperinsulinemia contributes to large vessel atheroschlerosis whether or not glucose intolerance exists.
Researchers believe that insulin resistance is caused by abnormalities within cells called post-binding abnormalities. • Many individuals with insulin resistance are deficient in a glucose transporter called a GLUT-4. • GLUT-4 is regulated by the amount of insulin present in the body.
Insulin Resistance and Thrifty Phenotype Hypothesis • Hypothesis—poor nutrition in fetal and infant life is believed to impair the normal development and function of beta cells as well as insulin-responsive tissues primarily in the skeletal muscle causing the development of insulin resistance
Maternal diabetes, high and low birth weights and the later development of diabetes has been reported in Pima Indians. • This suggests that high birth weight influences the development of insulin resistance as much as fetal underdevelopment
Predictors or Insulin Resistance--Adults • BMI of 25 or higher • Waist circumference >40 inches in men and 35 inches in women • Triglyceride >150 • HDL-C <40 • Blood pressure >130/85 • Fasting blood glucose >110 • Although these are adult references many practitioners use these values along with other predictors as possible clinical signs of insulin resistance
According to Hansen, Fulop and Hunter studies for children should include • Fasting blood glucose • Fasting insulin • Lipoproteins • Cortisol • Free T4 • TSH (thyroid stimulating hormone • Serum acetone • HbA1c • Urinalysis of glycosuria and ketonuria
Karotype and specialized genetic studies may be necessary if unusual phenotypic features are present to suggest chromosomal syndrome that may be associated with insulin resistance • Radiograph of the left hand and wrist may be indicated to assess bone age since insulin resistance in children is associated with advanced skeletal maturation.
Acanthosis nigricans • Result of hyperinsulinemia (consequence of insulin resistance • Caused from the binding of insulin to insulin-like growth factor receptors on keratinocytes and fibroblasts which results in hyperplasia of the skin
Causes light brown to black velvety rough areas typically at the base of the neck and skin folds • May be seen over joints including elbow, knees and knuckles or on the face and palms • 60-90% of children who develop diabetes have acanthosis nigricans • It is helpful clinical sign because it is truly a manifestation of insulin resistance
Insulin Resistance Syndrome • Characterized by hyperinsulinemia and one or more of the following • HTN • Hypertriglyceridemia • Hypercholesterolemia • Decreased HDL, Increased LDL • Obesity • Menstrual disturbances • Hirsutism
Insulin Resistance • Seen as early as 2 years of age in children with with appropriate genes, and environmental influences (ethnicity, obesity, decreased activity • Most common in puberty secondary to increased growth hormone secretion • Higher rate among African Americans, Hispanics and American Indians • Seen across all racial boundaries with increased obesity
Both parents obese the child has 66% chance of developing obesity • 50% chance if one parent is obese • Hyperinsulinemia contributes to development of obesity and obesity exacerbates insulin resistance • Insulin stimulates the appetite due to its anabolic mechanisms
Obesity and high body fat mass decrease insulin sensitivity in skeletal muscle and liver • Children usually begin to develop body fat mass in preschool years • Obesity is the most significant risk factor for developing insulin resistance
Obesity • In the last 30 years the % of young people who are overweight has doubled • 10-15% of children 6-17 years are overweight • 40% of obese 7 year olds and 70% of obese adolescents become obese adults
Physical activity • On a steady decline • Many children live in single parent or dual working households—more latchkey kids
Television • Many children begin watching TV as early as 6 months and are regular viewers by age 2. • American children watch TV for an average of 4 hours a day—2400 hours in one year • More time spent watching TV, computer and video games and less time in physical activity
Fast Food • On any given ay 7% of the American population eats fast food. • Today’s children have grown up in the era of “enhanced portion size” • Typical fast food mal is high in calories, fat and sugar • Even though families may choose to eat from home many rely on pre-processed “fast food” equivalents purchased at the grocery store because of lack of time to prepare a meal from scratch
Treatment • Alteration in lifestyle including modifications of • Eating habits • Increased physical activity • Prevention—curb the incidence of childhood obesity
Educational efforts targeted at the eating habits of both parents and children • Requires significant family involvement • May benefit from multidisciplinary approach from: primary care physician, RD or CDE, school personnel, psychologist
MNT remains the mainstay in treatment • Regimen used most often by pediatric diabetes dietitians is a variation of CHO counting • Reductions in calories and recommendations of 50% CHO, 20% protein and 30% fat • Fixed amount of CHO at each meal and snack
Physical activity increases the body’s sensitivity to insulin during activity and up to one day after activity • Studies show that regular aerobic exercise can reduce the risk of developing diabetes by 1/3 to ½ • Encourage daily with a sustained heart rate of 80% of maximum for 20-30 minutes
Children should be encouraged to participate in activities they can perform easily and frequently • Helpful if physical activity is “family centered”
Pharmacalogical Agents • Under exploration in the treatment of insulin resistance • Thiazolidionediones (TZD’s) directly address insulin resistance • They enhance glucose transport into target cells (especially muscle and adipose tissue)
TZD’s activate the peroxisome-proliferator receptor-gamma which stimulates a genetic transcription factor that enhances production of GLUT-4 • Many individuals with insulin resistance are deficient in GLUT-4
Biguanides (Metformin) inhibit glucose release from the liver by blocking gluconeogenesis and glycogenolysis • Biguanides associated with weight loss
There are no specific guidelines for using pharmacological agents in the treatment of insulin resistance • Specifically none of these medications have been sanctioned by the FDA to use in children • Given the prominence of insulin resistance and pathophysiology it is logical to theorize that reduction of insulin resistance before the development of diabetes may at least delay its occurrence
Recommendations • Canadian Pediatric Society position statement for all health care professionals to promote healthy active living for all family members
Highlights of recommendations • Inquire about eating habits and physical activity at all health care visits • Promote consumption of fiber rich foods instead of high fat high sugar foods • Encourage to spend 30 minutes every day in physical activity • Counsel families to reduce sedentary lifestyles—limit exposure to TV, video or computer games
Encourage parents to be positive role models and incorporate physical activities all family members can do together • Advise parents to enroll their children in age and developmentally appropriate recreational activities
Advocate • Initiatives to serve healthy foods and eliminate the sale of high CHO soft drinks and high fat/sugar snacks in schools • Policies to reduce the sale of over-sized fast foods • Initiatives that provide children with quality daily physical education classes and use of school facilities after school
Community sport and recreation programs • Construction of safe recreation facilities, parks and playgrounds • Physical education throughout all age groups in all schools • Allocation of funding for research in the prevention of childhood obesity
Oklahoma State Department of Health-Chronic Disease Service-Recommendations • All overweight children with 2 other risk factors tested for diabetes at the onset of puberty (random bs or 8h fasting bs) • If tests negative but remains high risk, test annually thereafter with aggressive lifestyle modifications • Treat HTN, dyslipidemia, etc aggressively and evaluate yearly • Families should be counseled on eating habits that maintain normal body wt and 30 minutes of daily physical activity as a family lifestyle
Conclusion • Certain genes predispose certain people to develop insulin resistance, but other factors—inactivity, wt gain trigger insulin resistance • Treatment is change in lifestyle • Treatment must include the family and a team effort with healthcare professionals