Download
1 / 12
120 likes | 268 Views
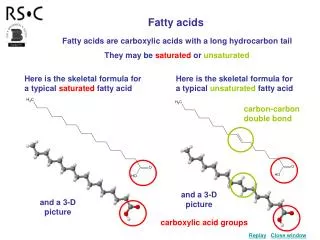
n-3 Fatty Acids in Patients with Multiple Cardiovascular Risk Factors. Christopher Paul Mckneely 2014 Doctor of Pharmacy Candidate Preceptor: Dr. Ali Rahimi. Background.

E N D
n-3 Fatty Acids in Patients with Multiple Cardiovascular Risk Factors Christopher Paul Mckneely 2014 Doctor of Pharmacy Candidate Preceptor: Dr. Ali Rahimi
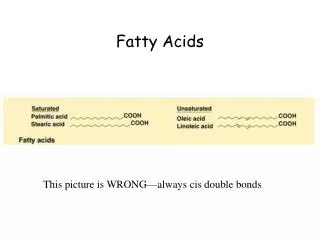
Background • n-3 derived fatty acid from fish (EPA/DHA) reduce the risk of cardiovascular disease by means of positive events on arrhythmic, atherosclerotic, inflammatory, and thrombotic processes. • Reduction in cardiovascular morbidity and mortality has been well documented in post-MI patients and heart failure patients.2 • This study looked into patients who had NO history of MI
Methodology • Risk and Prevention study • ongoing large-scale, multicenter, randomized, double-blind, placebo-controlled clinical trial conducted in the setting of Italian general practice1 • 860 General Practitioners • Steering Committee2 • Planning and coordinating • Analyzing and interpreting • Prepared the manuscript – submitted for publication • Baseline Characteristics of the patients • X2 for categorical variables • T-test or nonparametric test for continuous data • ANOVA used for comparison of multiple groups • BP, glucose, lipids, etc.
Methodology continued • Study participants2 • Men and women who met the inclusion criteria • Multiple cardiovascular risk factors • Clinical evidence of atherosclerotic vascular disease • Exclusion criteria • Previous MI, hypersensitivity to treatment, pregnancy, clinical conditions with poor short term prognosis or they can not give informed consent • 11,200 participants • Power of 90% • Alpha level of 0.05 • Would give 1383 events based off of primary end point – continued until all prescribers could recruit
Methodology continued2 • Study Procedure • Assigned to receive 1g of the fatty acids daily (content not <85%) or placebo (olive oil) • 12,513 patients total • 6239 in treatment group • 6266 in control or olive oil placebo group • Essential elements collected at baseline and at the patients yearly follow-up • Anthropometric, vitals, lifestyle habits, any new cardiovascular diagnosis, compliance and if the patient stopped the treatment for any reason • End points • Primary (expected to be 2%/year) • Rate of death, non-fatal MI/stroke • After one year (due to event rate lower than expected) • Composite of time to death from cardiovascular causes or hospitalizations due to cardiovascular causes • Secondary • Original primary end point
Statistics2 • Intent to treat population for primary end point • 1478 patients experienced the primary end point • 733 in treatment group (fatty acids) • 745 in placebo (olive oil) • Hazard ratio of 0.97, CI 95%, odds ratio 0.88-1.08, P=0.58 • Relative Risk Reduction of 15% stated (assumed) • Calculated (first relative risk) • RR = (a/(a+b))/(c/(c+d)) 0.98 • RRR = 1-RR or 1-.9837 .016 • ARR • Primary end point was met in 11.7% of pts on fatty acids and 11.9% who received placebo • 733 of 6239 in treatment had primary end point • 745 of 6266 in the placebo group had the primary end point • Calculated • CER- EER or 11.9%-11.7% -- 0.2% • NNT/NNH • 1/ARR = 500 NNT
Statistics2 • Per protocol • Protocol was for those who did NOT stop the treatment regimen • 1115 pts stopped treatment in the fatty acid arm • 1218 pts stopped treatment in the placebo arm • 10,172 remained were treated as per protocol • 527 in treatment group experienced primary end point (10.3%) • 510 in placebo group experienced primary end point (10.1%) • Hazard ratio 1.01, Ci 95%, odds ratio 0.89-1.14, P=0.89 • Missing data for 22 patients was noted
Statistics2 • Cox proportional-hazard models used to analyze the treatment effect study end points2
Discussion • Randomized trial of n-3 fatty acids in a large population of patients with multiple cardiovascular risk factors • Patients had NO history of myocardial infarction • On the basis of the results… • Conclude that there was no significant benefit of n-3 fatty acids in reducing risk of death from cardiovascular causes or hospital admissions for cardiovascular causes
Recommendation3 • Dietary recommendation for a specific amount of n-3 fatty acids is not being made • In the view of the ATP III panel, more definitive clinical trials are required before relatively high intakes of n-3 fatty acids (1–2 g/day) can be strongly recommended for either primary or secondary prevention.
References • 1. Rischio and Prevenzione Investigators. Efficacy of n-3 polyunsaturated fatty acids and feasibility of optimizing preventive strategies in patients at high cardiovascular risk: rationale, design and baseline characteristics of the Rischio and Prevenzione study, a large randomised trial in general practice. Trials. 2010; 11:68. doi: 10.1186/1745-6215-11-68. Accessed May 23, 2013. • 2. The Risk and Prevention Study Collaborative Group. n-3 Fatty acids in Patients with Multiple Cardiovascular Risk Factors. NEJM. 2013;368:1800-1808. • 3. National Cholesterol Education Program Expert Panel on Detection Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106:3143–421.