Download
1 / 16
160 likes | 261 Views
C omparative Effectiveness: A Manufacturer’s Perspective. AHRQ 2007 Annual Conference September 27, 2007. Peter Juhn, MD, MPH Vice President Evidence and Regulatory Policy Johnson & Johnson Corporate Office New Brunswick, NJ 732-524-6484. Evolving Environment . Challenges.

E N D
Comparative Effectiveness: A Manufacturer’s Perspective AHRQ 2007 Annual Conference September 27, 2007 Peter Juhn, MD, MPH Vice President Evidence and Regulatory Policy Johnson & Johnson Corporate Office New Brunswick, NJ 732-524-6484
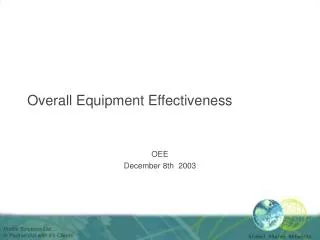
Evolving Environment Challenges Drivers Activities Policies Comparative Effectiveness Practice Variation Cost • Coverage and Reimbursement • Evidence Review • Quality Measurement • Insurance Benefit Design • HIT – EMR, PHR, Data Mining Coverage with Evidence Development Aging Population Access to and Payment for Innovative and effective products Quality/Safety Rising Demand Pay-for- Performance Cost of Technology Value Benefit-Risk Determination Budget Pressures
Healthcare Stakeholders Manufacturers Payers/ Regulators Pharmaceutical Medical Devices Distributor/Wholesaler Biotech Employer Other Payer Outpatient LTCFacilities Hospitals Physicians RegulatoryAgency IntegratedNetworks Patients Providers
Healthcare Stakeholders Manufacturers Payers/ Regulators Pharmaceutical Medical Devices Distributor/Wholesaler Biotech Employer • Patient – “am I getting the best care?” • Convenient • Respectful/compassionate • Trusted information about choices • Lower out-of-pocket cost Other Payer Outpatient LTCFacilities Hospitals Physicians RegulatoryAgency IntegratedNetworks Patients Providers
Healthcare Stakeholders • Provider – “am I being rewarded for good work?” • Better outcomes • Higher reimbursement • Increased volume • More efficiency • Chance to innovate • Enhanced reputation Manufacturers Payers/ Regulators Pharmaceutical Medical Devices Distributor/Wholesaler Biotech Employer Other Payer Outpatient LTCFacilities Hospitals Physicians RegulatoryAgency IntegratedNetworks Patients Providers
Healthcare Stakeholders Manufacturers Payers/ Regulators Pharmaceutical Medical Devices Distributor/Wholesaler Biotech Employer Other Payer Outpatient LTCFacilities Hospitals • Employer – “am I getting value for money?” • Lower cost • “Best care” • Not unhappy beneficiaries/workforce • Healthy productive employees Physicians RegulatoryAgency IntegratedNetworks Patients Providers
Healthcare Stakeholders Manufacturers Payers/ Regulators Pharmaceutical Medical Devices Distributor/Wholesaler Biotech Employer Other Payer Outpatient LTCFacilities Hospitals Physicians • Payer – “am I only paying for effective care?” • Lower cost • Predictability • Better outcomes (influence on later costs) RegulatoryAgency IntegratedNetworks Patients Providers
Healthcare Stakeholders Manufacturers Payers/ Regulators Pharmaceutical Medical Devices Distributor/Wholesaler Biotech Employer Other Payer Outpatient • Regulator – “am I protecting the public health?” • Safe and effective products • Two types of challenges: • Approving a drug later found to be dangerous • Not approving a useful drug in a timely fashion LTCFacilities Hospitals Physicians RegulatoryAgency IntegratedNetworks Patients Providers
Healthcare Stakeholders Manufacturers Payers/ Regulators Pharmaceutical Medical Devices Distributor/Wholesaler Biotech Employer Other Payer Outpatient LTCFacilities • Manufacturer – “am I being rewarded for safe and effective products?” • Improved patient outcomes • Recoup R&D investments • Fair and transparent coverage process • Clear evidence requirements Hospitals Physicians RegulatoryAgency IntegratedNetworks Patients Providers
Key Questions about Products • Does it work? Is it safe? • Regulatory Approval • Relevant for covered population (i.e. Medicare over 65y) • When should it be used? Who will most benefit? • Appropriateness guidelines • Patient selection criteria • How does it compare? Is it definitively better? • Earlier generation of technology • Within same class of technology • Rigor of comparative reviews • What is the value? Can the value be captured? • Is it cost-effective? Is it cost-saving? • Is there an ROI? When? To Whom?
Evidence Challenges • Availability of evidence • Needs for evidence are increasing • Large gaps in the existing literature • Limited generalizability of trials data to real-world practice • Unique challenges of devices • Distinguishing operator vs. product effects • Short product life-cycles • Feasibility of RCTs • Conclusions from the evidence • Reconciling “average” population effects with individual effects • “Shelf-life” of evidence • Practical use of evidence • Application of evidence to real-world medical decisions • Provider “accountability” for using evidence
The Promise of EBM • Properly developed and applied, evidence-based medicine can: • Stimulate the development of high quality information about treatments and devices • Enhance consistent and informed healthcare decision-making by physicians, patients, caregivers and payers • Support patient access to appropriate technologies • Help establish the value of medicines, medical devices, diagnostics and other health services • Provide the basis for optimal use of health care resources • Promote a more quality-focused and cost-effective healthcare system that delivers superior patient outcomes
The Perils of EBM • Potential for unintended consequences • Justifies coverage decisions based purely on cost without regard for overall effectiveness or value • Freezes the pace of innovation to the current generation of products • Discriminates against new technologies • Leads to prescriptive clinical protocols that do not allow for physician judgment and consideration of patient preferences • Focuses too narrowly on clinical morbidity or mortality, ignoring a range of other important patient-reported outcomes (ease of use, compliance, functional status) • Changes to coverage policies occur haphazardly without clear rationale, transparency or accountability
Comparative Effectiveness • What is J&J’s position on comparative effectiveness? • Help establish the value of treatments • Promote a more quality-focused cost-effective health system • Help physicians and patients make better decisions • Be a way for manufacturers to differentiate products • However, it is not the “silver bullet” as it will not automatically solve our cost and quality challenges • How should information from CE research be used? • Should inform medical decisions, not replace medical judgment with treatment formulas • Will need to reconcile “average” population effects and with impacts on individuals that reflect differences in side effects, intolerance, noncompliance, and quality of life
Comparative Effectiveness • How should it be linked to coverage decisions by payers? • Should not serve the cost containment concerns of payers • Might be most useful in informing treatment options and assigning appropriate reimbursement premiums • How should this information be communicated? • Share widely with all stakeholders, particularly providers and patients • Consider the dangers of incomplete understanding of results, particularly when communicated in an overly simplistic manner • Acknowledge that CE information can be incomplete, misleading, or misinterpreted • How should stakeholders be involved? • Participate in framing the methods that will be used and prioritizing the key therapeutic areas • Promote transparency about the processes, findings, limitations, and appropriate uses of the information
A Few Suggestions • Definitions • Comparison of “what to what” • Drug to drug; drug to procedure; disease management to not • What will success look like – information output vs. impact on care delivery • Scope • Clinical decision dilemmas vs. population economics • Synthesis of current evidence vs. initiating new comparative research • Funding • Commitment to conduct adequately powered studies • Distance from payment authorities • Stakeholders • Genuine involvement with priority setting, methods review and communication approaches