Download
1 / 59
750 likes | 3.35k Views
Disease of external nose. BY- KCSUDEEP. Cellulitis. The nasal skin may be invaded by streptococci or staphylcocci leading to a red, swollen and tender nose sometimes , it is an extension of infection from the nasal vestibule. Treatment

E N D
Disease of external nose • BY- KCSUDEEP
Cellulitis • The nasal skin may be invaded by streptococci or staphylcoccileading to a red, swollen and tender nose sometimes, it is an extension of infection from the nasal vestibule. Treatment • Systemic antibacterials hot fomentation and analgesics.
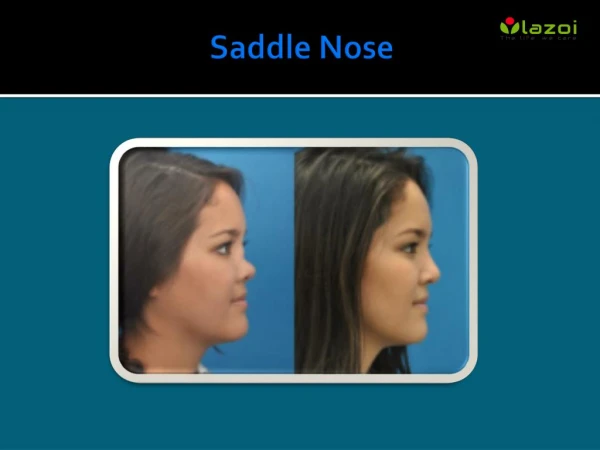
Nasal deformities Saddle nose • Depressed nasal dorsum may involve bony, cartilaginous or both bony and cartilaginous components of nasal dorsum. Nasal trauma causing depressed fractures is the most common aetiology.
It can also result from excessive removal of septum in submucous resection , destruction of septal cartilages by haematoma or abscess, sometimes by leprosy, tuberculosis or syphilis. • The deformity can be corrected by augmentation rhinoplasty by filling the dorsum with cartilage, bone or a synthetic implant. • If depression is only cartilaginous, cartilage is taken from the nasal septum or auricle and laid in a single or multiple layers. • If deformity involves both cartilage and bone, cancellous bone from the iliac crest is the best. Auto grafts are preferred to allografts . • Saddle deformity can also be corrected by synthetic implants of silicone or Teflon but they are likely to be extruded.
Hump nose this may also involve the bone or cartilage or both bone and cartilage. • It can be corrected by reduction rhinoplasty which consists of exposure of nasal framework by careful raising of the nasal skin by a vestibular incision , removal of hump and narrowing of the lateral walls by osteotomies to reduce the widening left by hump removal.
Crooked or a deviated nose • the midline of dorsum from frontonasal angle to the tip , is curved in a C or S shaped manner. In a deviated nose , themidline is straight but deviated to one side. • Usually ,these deformities are traumatic in origin . injuries sustained during birth, neonatal period or childhood, but not immediately recognized. Will also develop into these deformities with the growth of nose. • The deviated or crooked nose can be corrected by rhinoplasty or septorhinoplasty. Aim of these operations is to correct not only the outer appearance of nose but also its function .
TUMOURS • THEY MAY BE CONGENITAL , BENIGN OR MALIGNANT • 1.CONGENITAL TUMOURS Dermoid cyst • Simple dermoid:- it occurs as a midline swelling under the skin but in front of the nasal bones. It does not have any external opening. • That associated with a sinus:- it is seen in infants and children and is represented by a pit or a sinus in the midline of the dorsum of nose. Hair may be seen protruding through the sinus opening these cases, the sinus track may lead to a dermoid cyst under the nasal bone in front of upper part of the nasal septum a combined neurosurgical otolaryngologic approach is required in those extending intracranially so as to close simultaneously any bony defect through which the fistulous tract passes
ENCEPHALOCELE OR NINGOENCEPHALOCELE. • It is a herniation of brain tissue with meninges through a congenital bony defect. An extranasalmeningoencephalocele presents as a subcutaneous pulsatile swelling in the midline at root of nose ( naso frontal variety ), side of nose (nasoethmoid variety ) or on anteromedial aspect of the orbit ( naso-orbital variety). • Swellings show cough impulse and may be reducible. Treatment is neurosurgical: severing the tumour stalk from the brain and repairing the bony defect through which herniation has taken
Glioma- it is a nipped off portion of encephalocele during embroyonic development. MOST OF THEM (60% ) are extranasal and present as firm subcutaneous swellings on the bridge, side of nose or near the inner canthus. Some of them are purely in tranasal (30%) while 10% are both intra and extra nasal. Extranasalgliomas are encapsulated and can be easily removed by external nasal approach
Benign tumours • They arise from the nasal skin and include papillona , haemangioma, pigmented naevus • Seborrhoeickeratios • Neurofibroma • Or tumour of sweat glands.
Rhinophyma or potato tumour is a slow-growing benign tumour due to hypertrophy of the sebaceous glands of the tip of nose often seen in cases of long-standing acne rosacea. It presents as a pink , lobulated mass over the nose with superficilal vascular dilation : mostly affects men past middle age. • Patient seeks advice because of unsightly appearance of the tumour. Or obstruction in breathing and vision due to the large size of the tumour .
Treatment consists of paring down the bulk of tumour with sharp knife or carbon diaoxide laser and the area allowed to re-epithelialise. Sometimes, tumour is completely excised and the raw area skin-grafted.
MALIGNANT TUMOUR • Basal cell carcinoma ( rodent ulcer ) • Squamous cell carcinoma • Melanoma
TYPES:- • Nodular Papule or nodule, translucent or “pearly” • Ulcerating Ulcer (often covered with a crust)with a rolled border (rodent ulcer) • Cicatricial BCCs appear as scars • Superficial multicentric BCC appear as thin.Pink or red; characteristic fine threadlike telangiectasia can be seen with the aid of a hand lens. • Pigmented BCC may be brown to blue or black Smooth, glistening surface; hard, firm;cystic lesions may occur, however. Round, oval,shape, depressed center (“umbilicated”).
Causes • Skin cancer is divided into two major groups: nonmelanoma and melanoma. Basal cell carcinoma is a type of nonmelanoma skin cancer, and is the most common form of cancer in the United States. According to the American Cancer Society, 75% of all skin cancers are basal cell carcinomas.
Basal cell carcinoma starts in the top layer of the skin called the epidermis. It grows slowly and is painless. A new skin growth that bleeds easily or does not heal well may suggest basal cell carcinoma. The majority of these cancers occur on areas of skin that are regularly exposed to sunlight or other ultraviolet radiation. They may also appear on the scalp. Basal cell skin cancer used to be more common in people over age 40, but is now often diagnosed in younger people.
Your risk for basal cell skin cancer is higher if you have: • Light-colored skin • Blue or green eyes • Blond or red hair • Overexposure to x-rays or other forms of radiation • Basal cell skin cancer almost never spreads. But, if left untreated, it may grow into surrounding areas and nearby tissues and bone.
Symptoms • Basal cell carcinoma may look only slightly different than normal skin. The cancer may appear as skin bump or growth that is: • Pearly or waxy • White or light pink • Flesh-colored or brown • In some cases the skin may be just slightly raised or even flat. • You may have: • A skin sore that bleeds easily • A sore that does not heal • Oozing or crusting spots in a sore • Appearance of a scar-like sore without having injured the area • Irregular blood vessels in or around the spot • A sore with a depressed (sunken) area in the middle
Treatment Treatment varies depending on the size, depth, and location of the basal cell cancer. It will be removed using one of the following procedures: • Excision cuts the tumor out and uses stitches to place the skin back together. • Curettage and electrodesiccation scrapes away the cancer and uses electricity to kill any remaining cancer cells. • Surgery, including Mohs surgery, in which skin is cut out and immediately looked at under a microscope to check for cancer. The process is repeated until the skin sample is free of cancer. • Cryosurgery freezes and kills the cancer cells. • Radiation may be used if the cancer has spread to organs or lymph nodes or for tumors that can't be treated with surgery. • Skin creams with the medications imiquimod or 5-fluorouracil may be used to treat superficial basal cell carcinoma.
DIFFERENTIAL DIAGNOSIS • Solar keratosis • Bowen’s disease • Viral warts • Cutaneous horn • Keratoacanthoma • Basal cell carcinoma • Leg ulcers
Prognosis • The rate of basal cell skin cancer returning is about 1% with Mohs surgery, and up to 10% for other forms of treatment. Smaller basal cell carcinomas are less likely to come back than larger ones. Basal cell carcinoma rarely spreads to other parts of the body. • You should follow-up and regularly examine your skin once a month, using a mirror to check hard-to-see places.
Squamous Cell Carcinoma • From keratinizing or malpighian (spindle) cell layer of epithelium • Older, men, fair, blue-eyed, North European • Solar radiation (occupations) > chemicals, chronic ulcers, cytotoxic drugs, immunosuppressant drug treatment, dermatoses, discoid lupus, hidradenitis suppurativa • Xeroderma pigmentosum, albinism
Squamous Cell Carcinoma • Sun-exposed areas • Inflammation and induration with thickening beyond the clinical lesion presage the malignant transformation of a precancerous lesion into SCC • Types: • Slow-growing: Verrucous, exophytic, metastasizes • Rapid growing: Nodular, indurated, ulceration, invasive
Squamous Cell Carcinoma • Squamous epithelial cells invade the dermis with well-differentiated keratinization • Keratin pearls surrounded by epithelial cells • If poorly differentiated keratinization and inflammation are minimal or absent • Intercellular bridges are absent • Poorly differentiated lesions may have a pseudoglandular appearance
Squamous Cell Carcinoma • Small, isolated skin ulcerations treated conservatively for 2-3 weeks (ointment) • Treatment depends on size and patient age • Treatment options as for BCC (surgery/MMS) • Older patients treated conservatively • Recurrent lesion best treated by excision and grafting instead of a flap
Squamous Cell Carcinoma • MMS good for difficult or recurrent lesions especially in medial canthal and alar regions • Radiation can be effective in patients > 55 especially around eyes, nose and lips • ELND are not necessary
Squamous Cell Carcinoma • Mohs Micrographic Surgery • Good for genital tumors (v. amputation) • Early SCC of digits without bony involvement especially in periungual region to avoid amputation without compromising cure • Good for SCC in scar or radiation site due to high recurrence rate • Good for SCC in perineural or scalp
Squamous Cell CarcinomaPrognosis • 5-10% metastasize • Marjolin’s ulcer or xeroderma lesions more • Scalp lesions where there was previous radiation are prone to metastasize • Tendency for recurrence treated by any technique is twice that of BCC
Follow-up Treatment SCC • Clinically examined every 6 months for 5 years • 36% will develop second BCC in 5 years • Early diagnosis and treatment are important in recurrent lesions • SCC should be examined every 3 months for the first several years then indefinitely at 6 month intervals
Periodic Self Exam • Prevention is the best weapon • Curable disease if diagnosed early • Full-length mirror, hand mirror, well-lit room • Examine body front and back in mirror then R and L sides • Bend elbows and look at forearms, back of upper arms and palms • Back of legs and feet, b/w toes, soles • Neck, scalp, back and buttocks with hand mirror
melanoma • Least common variety • May be nodular or superficial spreading type .
This is an example of melanoma or malignant melanoma. This is the most dangerous form, and also the most rare.
The ABCD Rule of Melanoma • A = Asymetry – one half of the mole does not match the other • B = Border Irregularity – the edges of the mole are uneven, notched or blurred • C = Color – the pigment is not even. Cancerous moles may have several colors in one mole (blue, red, brown or black) • D = diameter - watch moles the size of a pencil eraser or larger for changes.
This melanoma grew under this man’s fingernail. The nail has been removed to facilitate removal of the tumor.
The large brown mass on the side of this woman’s nose is a malignant melanoma.
This is the same woman. Her melanoma has been removed. If you look closely, you can see the depression where the tumor once was located.
Doctors found that her cancer had spread, so she underwent chemotherapy to try to obliterate all of the cancerous cells. The differences in the woman’s appearance are side effects of the chemotherapy.
It’s hard to see what is wrong with this woman. There is a melanoma on the right side of her nose in this picture. Although it’s not dark, the tumor is still melanoma.
The woman’s nose had to be removed because the cancer was so advanced. The pen marks are guides for radiation, while the mouth cork is to keep her airway open.