Download
1 / 26
260 likes | 304 Views
The Sphenopalatine Ganglion (SPG) and Maxillo-Facial Health. Dietrich K.Klinghardt, MD, PhD Bellevue, WA tel: 425 637 9339 www.neuraltherapy.com Presented at the 23 rd Annual International Symposium on Man and His Environment June 9-12, 2005, Dallas, Tx

E N D
The Sphenopalatine Ganglion (SPG) and Maxillo-Facial Health Dietrich K.Klinghardt, MD, PhD Bellevue, WA tel: 425 637 9339 www.neuraltherapy.com Presented at the 23rd Annual International Symposium on Man and His Environment June 9-12, 2005, Dallas, Tx American Environmental Health Foundation
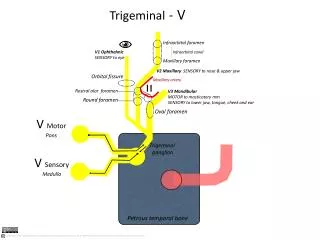
Anatomy/location: • aka: nasal ganglion, Meckel’s ganglion, pterygopalatine ggl. • Size/ Appearance: 6-8 mm, flattened, reddish-grey • Outside the cranial bowl • Adjacent to the cranium near the sphenopalatine foramen • Deeply in the sphenopalatine fossa • Cranial to the mandibular nerve • Close and lateral to (and below) the maxillary nerve (as it crosses the fossa) • 4 branches: orbital, palatine, nasal, pharyngeal
Neurology 1. Nerve fibers leading into the SPG • sensory nerve supply: via the sphenopalatine nerve and the maxillary nerve (establishing a strong “fine-fiber”connection between trigeminal fibers and parasympathetic fibers inside the ganglion) • Trigeminal fiber collaterals storing substance P in the sphenopalatine ganglion of the rat. An axon reflex modulating parasympathetic ganglionic activity? Suzuki N et al.; Neuroscience 1989;30(3): 595-604
Neurology • Parasympathetic: Connection from the vagus nerve and the 3 vagal ganglia in the brain stem. Parasympathetic nerves traveling piggyback on the N.petrosus major and fibers of the facial nerve originating at the ganglia geniculi (establishing a connection to the 7th cranial nerve) • Sympathetic connection via the N.petrosus profundus (establishing a connection with the superior cervical ganglion and the SNS)
2.Nervefibers emerging from the SPG • Connection to the parasympathetic fibers of the submandibular gland, the lacrimal gland and the parotid gland • Connection to the ciliary ganglion and various functions of the eye • Connections to the inner ear • Connections to olfactory nerve and lingual nerve (smell and taste) • Connection to the arterial blood supply of the brain • Connection to the dental pulp and osteoblasts of the jaw bone
Physiology a. Secreto-motor function • Eustachian tubes • Larynx • Tonsils • Mucous membranes of nose and sinuses (incl. Sphenoidal- and ehtmoidal sinuses). Trigeminal and SPG parasympathic fibers synapse inside the SPG Origin and distribution of capsaicin-sensitive substance p-immunoreactive nerves in the nasal mucosa Lundblad L et al; Acta Oto-Laryngologica, 1983, 96 (5-6) 485-493 • Soft, hard palate and maxilla • Lacrimal gland • Saliva producing glands (together with otic ganglion) • Badtke and Mudra: Neuraltherapie: Lehrbuch und Atlas. Ullstein Medical 1998, pg 108-109 • Gray’s Anatomy(1986), pg 1235-1236
b. Major role of the SPG (and otic ganglion) in the regulation of the brain (newer findings based on histochemistry research) • Principle of method used: presence of Vasoactive Intestinal Polypeptide (VIP) and Choline Acetyltransferase (ChAT) indicate parasympathetic function. Presence of Substance P pain indicates sensory nerve fiber function • Connection from SPG to the internal carotid ganglion (considered an aberrant sphenopalatine ganglion with about 70 cells each) inside the carotid artery) • The intracranial portion of the internal carotid artery has fibers from SPG. Activation of these nerves causes edema, pain, dilatation, low grade encephalitis (cluster headache, ophthalmoplegic symptoms) • Anatomical basis for a parasympathetic and sensory innervation of the intracranial segment of the internal carotid artery in man. Suzuki N, Hardebo JE J Neurolo Sci 1991 July; 104(1): 19-31
The SPG is a major source for postganglionic parasympathetic fibers to the vascular beds of the cerebral hemispheres. Treating the SPG can increase brain blood flow • Selective electrical stimulation of postganglionic cerebrovascular parasympathetic nerve fibers originating from the sphenopalatine ganglion enhances cortical blood flow in the rat Suzuki N, Hardebo JE, Kahrstrom J, Owman C J Cereb Blood Flow Metab 1990 May; 10(3): 383-91 Abnormal cranial parasympathetic outflow from the SPG induces vasodilation of cerebral and meningeal blood vessels, enhances plasma protein extravasation and the release of pro-inflammatory mediators. It can mediate the intracranial hypersensitivity found in MCS patients and is often responsible for sensitizing central nociceptive neurons in the spinal trigeminal nucleus. • 2003 Wolff Award: Possible parasympathetic contributions to peripheral and central sensitization during migraine Yarnitzky D et al; Headache, 2003, 43 (7) 704-714
Fibers from the otic ganglion contribute to the innervation of the pial arteries • The pathway of parasympathetic nerve fibers to cerebral vessels from the otic ganglion in the rat Hardebo JE, Suzuki N J Auton Nerv Syst 1991 Oct; 36(1): 39-46
Postganglionic fibers from the SPG are involved in tone regulation of the cerebral vessels • The cerebrovascular parasympathetic innervation Suzuki N, Hardebo JE Cerebrovasc Brain Metab Rev 1993 Spring; 5(1):33-46 Cell bodies of the SPG project along the 7th and 9th cranial nerve to the middle cerebral artery • Cerebrovascular projections from the sphenopalatine and otic ganglia to the middle cerebral artery of the cat Walters B, Gillespie B Moskowitz A Stroke Vol 17, No3 1986
Fibers from the SPG and Otic ganglion innervate the dental pulp • Otic ganglion parasympathetic neurons innervate the pulp of the mandibular incisor or the guinea pig: Segade L, Suarez-Quintanilla D Neuroscience Letters 1988, 90(1-2) 33-38 • Local actions of acetylcholine on vasomotor regulation in rat incisor pulp Olgart L et al; Acta physiologica scandinavica 1996, 158(4) 311-316 • The excitatory action of acetylcholine on intradental sensory units • Maegerstam et al, Acta physiologica scand. 1975, 93(1) 113-118 • Occurrence of axons with certain immunohistochemical markers in teleost of gingival and teeth, Tuisku F, Hildebrand C, Brain Research, 1996, 729(1), 137-141 • Cat dental pulp after denervation and subsequent re-innervation: changes in blood flow regulation and distribution of neuropeptideY, GAP-43 and neurotrophin receptor-like immunoreactivity, Olgart L, Edwall L, Fired K; Brain Research 1993, 625(1) 109-119
Reported symptoms of SPG dysfunction prior to 1979 • Convulsive disorders pain of the head and neck facial pain • Muscle spasm of both voluntary and involuntary muscles • Rage reactions • Psychosomatic symptoms, including fatigue and extreme sensitivity • Blindness and glaucoma • Metallic taste • Ophthalmic migraine and herpes • “Lower half headache” • Abdominal pain • Diarrhea
Reported symptoms of SPG dysfunction prior to 1979 • Pain in shoulder and upper extremity, low back pain, sciatica • Asthma • Angina pectoris • Intractable hiccup • Menstrual pain • Hyper- and hypothyroidism • Nasal congestion, sneezing, tearing, photophobia, hayfever • Glossodynia, • Otalgia • Nausea • Sphenopalatine(nasal) ganglion: remote effects including “psychosomatic” symptoms, rage reaction, pain and spasm Ruskin A Arch Phys Med Rehabil Vol 60 Aug 1979 142-147
The SPG and MCS The superficial location in the pharynx explains the extraordinary sensitivity of this ganglion to odors, chemicals and particles in the air • Studies do not show increased sensitivity of the olfactory system but increased sensitivity/dysfunction of the parasympathetic system • Symptoms consistent with parasympathetic SPG- dysfunction induced by rose oil and a common solvent (methyl ethyl ketone) have been described in a study on 18 MCS patients (with a normal control group) • Decreased airway patency • Decreased pulse rate • Decreased blood pressure • Increased depression • No greater olfactory threshold sensitivity • Olfactory sensitivity, nasal resistance and autonomic function in patients with multiple chemical sensitivities Doty R et al; Arch Otolaryngol Head Neck Surg, Vol 114, Dec 1988, pg 1422 ff
The neighborhood to the teeth and parasympathetic innervations of the teeth suggests a vulnerability to mercury fumes escaping from dental amalgam fillings Patrick Stoertebecker, MD (neurologist at the Karolinska Institute) focused his research of retrograde axonal transport of mercury on the olfactory nerve and hypoglossal nerve, but observed rapid and severe contamination of the facial parasympathetic ganglia as well. • Mercury poisoning from dental amalgam – a hazard to the human brain Patrick Stoertebecker, Bio-Probe 1992 ISBN 0-941011-01-1
Using the neural therapy technique of injecting the SPG with DMPS has been found extremely valuable in the course of published detoxification protocols • Results of dental amalgam removal and mercury detoxification using DMPS and neural therapy Robert Kidd; Alternative Therapies, July 2000, Vol 6, No, 49-55 • Migraines, seizures and mercury toxicity Klinghardt, D and Leviton R; Alternative MedicineDigest Issue 21,1999, pg 63
The intricate connection to the vagus nerve and the contribution to the innervation of the saliva producing glands predicts many of the digestive symptoms observed in dysfunctional states of the SPG
The little explored access of the SPG to the deep cerebral arterial supply can explain many of the brain/limbic system related observations in MCS Many chemicals act as cholinesterase inhibitors, cause therefore disruption of normal parasympathetic function and can lead to dysfunction of the SPG • Neuropsychological effects of long-term exposure to pesticides: results from the French Phytoner study Baldi I et al; Environmental Health Perspectives Vol 109 No 8 Aug 2001 • A rat mammary tumor model induced by organophosphorus pesticides parathion and malathion, possibly through acetylcholinesterase inhibition Cabello G et al: Environmental Health Persepectives Vol 109, No5, May 2001
Sphenopalatine ganglion-related MCS symptoms • Exaggerated reactions to inhalants, foods and odors • Chronic sinusitis • Rhinitis • Eye problems • Tinnitus and high pitch hearing loss • Digestive problems • Facial pain and headache • Inappropriate emotional states • Cognitive problems of the brain • Fatigue
Diagnosis • Clinical: based on symptoms of dysfunctional SPG (Ruskin paper) • Thermography (abnormal warmth in the mandibular nerve distribution) • EDS/EAV • Autonomic response testing • Using the bi-digital o-ring test to detect dysfunction of the autonomic nervous system Klinghardt D; Program and abstracts 14th international symposium on acupuncture and electrotherapeutics. International J of Acup and Electrotherapeutics Res, Vol 23, No 3 and 4, 1998, 288-289
Treatment-options for the dysfunctional SPG • Injections a. techniques • intraoral approach medial to 2nd molar tooth (greater palatine foramen) • supra-zygomatic approach • Manual of Neural Therapy Peter Dosch, Haug Publishers Heidelberg, 1st English Edition 1984, pg 373-375I • llustrated Atlas of the Techniques of Neural Therapy with Local Anesthetics Mathias Dosch;Thieme 2002 (foreword by D. Klinghardt, MD PhD) b. injectible medications: preservative free ph-buffered procaine, saline, glutathione-SH, DMPS, phospholipids, Desferal, Ca-EDTA, vit. C, NAC, homeopathic preparations, ozone (Neural Therapy B, www.nerualtherapy.com)
Treatment-options for the dysfunctional SPG • Nasal applicator (Q-tip): 5% procaine, essential oils (nasosympatico, Wise Woman Herbals) • Sphenopalatine(nasal) ganglion: remote effects including “psychosomatic” symptoms, rage reaction, pain and spasm Ruskin A Arch Phys Med Rehabil Vol 60 Aug 1979 145-146 • The use of topical 4% lidocaine in sphenopalatine ganglion blocks for the treatment of chronic muscle pain syndromes : a randomized, controlled trial Scudds R A et al; Pain:(Amsterdam),1995, 62 (1) 69-77 • Possible parasympathetic contributions to peripheral and central sensitization during migraine ;2003 Wolff Award: Yarnitzky D et al; Headache, 2003, 43 (7) 704-714 • Micro-current (KMT technology). Intraoral electrode placement or external temporal approachwww.neuraltherapy.com • Cranio-sacral therapy (manual osteopathic therapy to the spheno-basilar junction and sphenoid bone) • Good structural dentistry: best for long term results
Results I have successfully treated more then 400 MCS clients (diagnosis was established by prior treating physicians) My approach includes • Life style changes (avoidance, exercise, sauna, meditation or prayer, amalgam/root filled tooth removal) • Diet changes (diet therapy software) • Treatment of chronic stealth infections • Mental field therapy (www.neuraltherapy.com) • intravenous therapies with glutathione, vitamin C, NAC and other detoxification strategies • oral orthomolecular program • bio-identical hormone replacement • neural therapy, including regular sphenopalatine ganglion “blocks”
Conclusion: Both the literature and clinical experiencesuggest that treating the sphenopalatine ganglion can be a rewarding, safe and lasting intervention in the treatment of environmental sensitivity and illness