Download
1 / 1
10 likes | 155 Views
Boston Keratoprosthesis – the Eye and Ear Experience J Brady, W Power The Authors have no financial interest in the subject matter of this poster Royal Victoria Eye and Ear Hospital, Dublin. Background

E N D
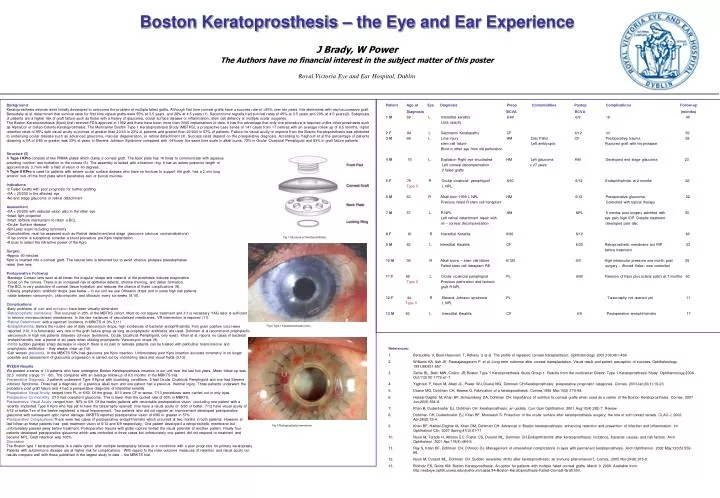
Boston Keratoprosthesis – the Eye and Ear Experience J Brady, W Power The Authors have no financial interest in the subject matter of this poster Royal Victoria Eye and Ear Hospital, Dublin • Background • Keratoprosthesis devices were initially developed to overcome the problem of multiple failed grafts. Although first time corneal grafts have a success rate of >95% over ten years, this diminishes with each successive graft. Bersudsky et al. determined that survival rates for first time repeat grafts were 55% at 3.5 years, and 28% at 4.5 years (1). Second time regrafts had survival rates of 45% at 3.5 years and 20% at 4.5 years(2). Subgroups of patients are a higher risk of graft failure such as those with a history of glaucoma, ocular surface disease or inflammation, stem cell defiency or multiple ocular surgeries. • The Boston Keratoprosthesis (Kpro) first received FDA approval in 1992 and there have been more then 3000 implantations to date. It has the advantage that only one procedure is required unlike other prostheses such as AlphaCor or Osteo-Odonto-Keratoprosthesis. The Multicenter Boston Type 1 Keratoprosthesis Study (MBTKS), a prospective case series of 141 cases from 17 centres with an average follow up of 8.5 months, report retention rates of 95% with visual acuity outcomes of greater than 20/40 in 23% of patients and greater than 20/200 in 57% of patients. Failure for visual acuity to improve from the Boston Keratoprosthesis was attributed to underlying ocular disease such as advanced glaucoma, macular degeneration, or retinal detachment (3). Success rates depend on the preoperative diagnosis. According to Yaghouti et al the percentage of patients obtaining a VA of 6/60 or greater was 33% at years in Stevens Johnson Syndrome compared with 64%over the same time scale in alkali burns, 72% in Ocular Cicatricial Pemphigoid and 83% in graft failure patients • Structure (5) • A Type I KPro consists of two PMMA plates which clamp a corneal graft. The back plate has 16 holes to communicate with aqueous • providing nutrition and hydration to the cornea (6). The assembly is locked with a titanium ring. It has an antero-posterior length of • approximately 3.7mm with a field of vision of 60 degrees. • A Type II KPro is used for patients with severe ocular surface disease who have no fornices to support the graft. has a 2 mm long • anterior nub off the front plate which penetrates skin or buccal mucosa. • Indications • 2 Failed Grafts with poor prognosis for further grafting • VA < 20/200 in the affected eye • No end stage glaucoma or retinal detachment • Assessment • VA < 20/200 with reduced vision also in the other eye • Intact light projection • Intact lid/blink mechanism to retain a BCL • Ocular Surface disease • Slit Lamp exam including tonometry • Comorbidities must be assessed such as Retinal detachment/end stage glaucoma (obvious contraindications) • If iop control is suboptimal consider a shunt procedure pre Kpro implantation • A scan to select the refractive power of the Kpro • Surgery • Approx 90 minutes • Kpro is inserted into a corneal graft. The natural lens is removed but to avoid vitreous prolapse pseudophakes • retain their lens. • Postoperative Followup • Bandage Contact lens worn at all times: the irregular shape and material of the prosthesis induces evaporative • forces on the cornea. There is an increased risk of epithelial defects, stromal thinning, and dellen formation. • The BCL is very protective of corneal tissue hydration and reduces the chance of these complications (8). • Lifelong prophylactic antibiotic drops (see below – in our unit we use Ofloxacin drops and in some high risk patients • rotate between vancomycin, chloromycetin and oflocacin every six weeks (9,10). • Complications • Early problems of melt and extrusion have been virtually eliminated • Retroprosthetic membrane: This occurred in 25% of the MBTKS cohort. Most do not require treatment and if it is necessary YAG laser is sufficient • to remove nonvascularised membranes. In the rare instances of vascularised membranes, VR intervention is required (11). • Retinal Detachment: with a reported incidence in MBKTS of 3% 3,11) • Endophthalmitis:Before the routine use of daily vancomycin drops, high incidences of bacterial endophthalmitis from gram positive cocci were • reported (10). It is fortunately very rare in the graft failure group as long as prophylactic antibiotics are used. Dohlman et al recommend prophylactic • vancomycin in high risk patients (Stevens Johnson Syndrome, Ocular Cicatricial Pemphigoid, only eyes). Khan et al. reports no cases of bacterial • endophthalmitis over a period of six years when utilizing prophylactic Vancomycin drops (9). • Vitritis sudden painless sharp decrease in vision.It there is no pain or redness patients can be treated with peribulbar triamcinolone and • prophylactic antibiotics – they always clear up (12). • Can worsen glaucoma. In the MBKTS 53% had glaucoma pre Kpro insertion. Unfortunately post Kpro insertion accurate tonometry is no longer • possible and assessment of glaucoma progression is carried out by monitoring discs and visual fields (3,13). • RVEEH Results • We present a series of 13 patients who have undergone Boston Keratoprosthesis insertion in our unit over the last five years. Mean follow-up was • 32.3 months (range 11 - 60). The compares with an average follow-up of 8.5 months in the MBKTS trial. • Preoperative Diagnosis: 3 patients underwent Type II Kpros with cicatrizing conditions. 2 had Ocular Cicatricial Pemphigoid and one had Stevens • Johnson Syndrome. Three had a diagnosis of a previous alkali burn and one patient had a previous thermal injury. Three patients underwent the • procedure post graft failure and 4 had a preoperative diagnosis of interstitial keratitis. • Preoperative Visual Acuity: ranged from PL to 6/60. Of the group, 8/13 were CF or worse. 7/13 procedures were carried out in only eyes. • Preoperative Co-morbidity: 2/13 had coexistent glaucoma. This is lower than the quoted rate of 60% in MBKTS. • Postoperative Visual Acuity: ranged from NPL to 6/9. Of the twelve patients with recordable postoperative vision (excluding one patient with a • recently implanted Type II Kpro who has yet to have the tarsarraphy opened) nine have a visual acuity of 6/60 or better. 7/12 have visual acuity of • 6/12 or better.Ten of the twelve registered a visual improvement. Two patients who did not register an improvement developed postoperative • glaucoma with subsequent optic nerve damage. MKBTS reported postoperative vision of 6/60 or greater in 57% • Postoperative Complications:There were two cases of postoperative endophthalmitis which occurred at two months in both patients. However at • last follow-up these patients had post treatment vision of 6/12 and 6/9 respectively. One patient developed a retroprosthetic membrane but • unfortunately passed away before treatment. Postoperative trauma with globe rupture limited the visual potential of another patient. Finally four • patients developed postoperative glaucoma which was controlled in three cases but unfortunately one patient did not respond to treatment and • became NPL. Graft retention was 100%. • Discussion • The Boston type 1 keratoprosthesis is a viable option after multiple keratoplasty failures or in conditions with a poor prognosis for primary keratoplasty. • Patients with autoimmune disease are at higher risk for complications. With regard to the main outcome measures of retention and visual acuity our • results compare well with those published in the largest study to date – the MBKTS trial. Patient Age at Eye Diagnosis Preop Comorbidities Postop Complications Follow-up Diagnosis BCVA BCVA (months) 1 M 69 L Interstitial keratitis 6/60 6/9 nil 40 Lens opacity 2 F 84 L Salzmamn Keratopathy CF 6/12 nil 39 3 M 68 L Lime injury HM Disc Pallor CF Postoperative trauma 38 stem cell failure Left amblyopia Ruptured graft with iris prolapse Blind in other eye from old perforation 4 M 70 L Explosion Right eye enucleated HM Left glaucoma HM Developed end stage glaucoma 23 Left corneal decompensation x 27 years 2 failed grafts 5 F 79 R Ocular cicatricial pemphigoid 6/60 6/12 Endophthalmitis at 2 months 26 Type II L NPL 6 M 63 RAlkali burn 1999 L NPL HM 6/12 Postoperative glaucoma 22 Previous failed R stem cell transplant Controlled with topical therapy 7 M 57 L R NPL HM NPL 6 months post surgery admitted with 50 Left retinal detachment repair with eye pain high IOP. Despite treatment oil – corneal decompensation developed pale disc 8 F 81 R Interstitial Keratitis 6/60 6/12 46 9 M 80 L Interstitial Keratitis CF 6/30 Retroprosthetic membrane but RIP 23 before treatment 10 M 36 R Alkali burns – stem cell failure 6/120 6/9 High intraocular pressure one month post 25 Failed stem cell transplant RE surgery – Ahmed Valve- now controlled 11 F 80 L Ocular cicatricial pemphigoid PL 6/60 Revision of Kpro plus scleral patch at 7 months 60 Type II Previous perforation and tectonic graft R NPL 12 F 44 R Stevens Johnson syndrome PL Tarsorraphy not opened yet 11 Type IIL NPL 13 M 62 L Interstitial Keratitis CF 6/9 Postoperative endophthalmitis 17 Fig 1 Structure of Keratoprosthesis Fig 2 Type I Keratoprosthesis in situ • References: • Bersudsky V, Blum-Haeuveni T, Rehany U et al. The profile of repeated corneal transplantaion. Ophthalmology 2001;108:461-469 • Williams KA, Ash JK, Pararajasegaram P, et al. Long-term outcome after corneal transplantation. Visual result and patient perception of success. Ophthalmology. 1991;98:651-657 • Zerbe BL, Belin MW, Ciolino JB; Boston Type 1 Keratoprosthesis Study Group.1: Results from the multicenter Boston Type 1 Keratoprosthesis Study. Ophthalmology.2006Oct;113(10):1779.e1-7. • Yaghouti F, Nouri M, Abad JC, Power WJ, Doane MG, Dohlman CH.Keratoprosthesis: preoperative prognostic categories. Cornea. 2001Jan;20(1):19-23. • Doane MG, Dohlman CH, Bearse G. Fabrication of a keratoprosthesis. Cornea.1996 Mar;15(2):179-84. • Harissi-Dagher M, Khan BF, Schaumberg DA, Dohlman CH. Importance of nutrition to corneal grafts when used as a carrier of the Boston Keratoprosthesis. Cornea. 2007 Jun;26(5):564-8. • Khan B, Dudenhoefer EJ, Dohlman CH. Keratoprosthesis: an update. Curr Opin Ophthalmol. 2001 Aug;12(4):282-7. Review. • Dohlman CH, Dudenhoefer EJ, Khan BF, Morneault S. Protection of the ocular surface after keratoprosthesis surgery: the role of soft contact lenses. CLAO J. 2002 Apr;28(2):72-4. • Khan BF, Harissi-Dagher M, Khan DM, Dohlman CH. Advances in Boston keratoprosthesis: enhancing retention and prevention of infection and inflammation. Int Ophthalmol Clin. 2007Spring;47(2):61-71 • Nouri M, Terada H, Alfonso EC, Foster CS, Durand ML, Dohlman CH.Endophthalmitis after keratoprosthesis: incidence, bacterial causes, and risk factors. Arch Ophthalmol. 2001 Apr;119(4):484-9. • Ray S, Khan BF, Dohlman CH, D'Amico DJ. Management of vitreoretinal complications in eyes with permanent keratoprosthesis. Arch Ophthalmol. 2002 May;120(5):559-66. • Nouri M, Durand ML, Dohlman CH. Sudden reversible vitritis after keratoprosthesis: an immune phenomenon?. Cornea. 2005 Nov;24(8):915-9. • Birkholz ES, Goins KM. Boston Keratoprosthesis: An option for patients with multiple failed corneal grafts. March 9, 2009. Available from: http://webeye.ophth.uiowa.edu/eyeforum/cases/94-Boston-Keratoprosthesis-Failed-Corneal-Graft.htm. Fig 3 Retroprosthetic membrane