Download

1 / 40
400 likes | 721 Views
Obesity & Anaesthesia. Dr Ikhwan Wan Mohd Rubi MD (UKM) MO Anaesthesiology , HSNZ. 1/6 Malaysians are either overweight/obese- Malaysia Ministry of Health .

E N D
Obesity & Anaesthesia DrIkhwan Wan MohdRubi MD (UKM) MO Anaesthesiology, HSNZ
1/6 Malaysians are either overweight/obese- Malaysia Ministry of Health
“Malaysia is leading in the prevalence of obesity among Southeast Asian countries. Almost one in two Malaysians are either overweight or obese, placing them at a high risk for diabetes,”saysDatinPadukaSanthaKumari, chairman of the Selangor branch of the Malaysian Diabetes Association.
Classical description of obesity Intraperiotenal fat (liver,omentum) Peripehral fat (arms,legs,buttock) Waist hip ratio: >0.94 in men >0.8 in women
Comorbid • BMI alone is a poor predictor of comorbidity, surgical and anesthetic difficulty • Fat distribution (waist/collar circumference) > predictive of CVS/Respiratory comorbid • Android fat distribution • Makes intra-abdominal surgery > difficult • Greater difficulty in airway management/ventilation • Greater risk of metabolic and CVS complication • Risk of comorbid increases the duration of obesity (fat years) • Presence and severity of comorbid may be masked by sedentary lifestyle • TRUE significance obesity related illness may only emerge during perioperative phase.
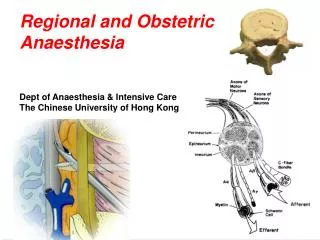
RESPIRATORY SYSTEM • OSA • Obesity Hypoventilation Syndrome • Airway Assessment • Obesity and gas exchange • Lung volume • O2 consumption and CO2 production • Gas exchange • Lung Compliance and resistance • Respiratory efficiency and work of breathing • Implication for anesthesia
CVS SYSTEM • Cardiovascular derangemnt • HPT • IHD • Blood Volume • Cardiac arrhythmia • Cardiac function
Obstructive Sleep Apnea • Up to 5% of obese patients have clinically significant obstructive sleep apnea • Apnea is defined as 10 seconds or more of total cessation of airflow despite continuous respiratory effort against a closed glottis
ObesityEffects on Blood Volume • Total blood volume is increased in the obese, but on a volume-to-weight basis, it is less than in nonobese individuals(50ml/kg compared to 70ml/kg) • Most of this extra blood volume is distributed to the fat organ
ObesityCardiovascular Effects • Cardiac output increases as much as 20 – 30 ml/kg of excess body fat secondary to ventricular dilatation and increasing stroke volume • The increased left ventricular wall stress leads to: • Hypertrophy • Reduced compliance • Impaired left ventricular filling • Obesity cardiomyopathy
ObesityEffects on Gastrointestinal System • Gastric volume and acidity are increased • Most fasted morbidly obese patients presenting for elective surgery have gastric volumes in excess of 25 ml and gastric fluid pH less than 2.5 ( the generally accepted volume and Ph indicative of high risk for pneumonitis should regurgitation and aspiration occur). • Gastric emptying may actually be faster in the obese, but because of their larger gastric volume (up to 75% larger), the residual volume is larger.
ObesityObesity and Diabetes • Impaired glucose tolerance in the morbidly obese is reflected by a high prevalence of type II diabetes mellitus as a result of resistance of peripheral fatty tissues to insulin • Greater than 10% of obese patients have an abnormal glucose tolerance test, which predisposes them to wound infection and an increased risk of myocardial infarction during periods of myocardial ischemia
ObesityEffects on the Airway • Anatomic changes that contribute to potential for difficult airway management • Limitation of movement of the atlantoaxial joint and cervical spine by upper thoracic and low cervical fat pads • Excessive tissue folds in the mouth and pharynx • Short thick neck • Suprasternal, presternal and posterior cervical fat • Very thick submental fat pad • Obstructive sleep apnea • Predisposes to airway difficulties during anesthesia • OSA patients have excess tissue deposited in their lateral pharyngeal walls which may not be recognized during routine airway examination
Preoperative Assessment(AAGBI/SOBA) • Obese patient may present for ELECTIVE/EMERGENCY surgery/ Obstetric Analgesic/Anesthesia • Similar between ELECTIVE/EMERGENCY • Multidiscipline- where deem necessary • Respiratory physician, Cardiologist, Endocrinologist, Dietitian • Specific attention to comorbid • Cardiovascular/Respiratory/Metabolic • Obese patient may have limited mobility, may appear relatively asymptomatic despite significant cardiorespiratory dysfunction
Preoperative Assessment (Respiratory) • Previous anesthetic experiences • Attention should focus on the cardiorespiratory system and airway • Assess for Obstructive Sleep Apnea and Obesity Hypoventilation Syndrome • STOP – BANG (5 or more) • Snoring (loudly) • Tired (often tired/sleepy at day time) • Observed (has anyone observed you stop breathing during sleep) • Pressure (has you been treated for/ has high blood pressure) • BMI>35kg/m2 • Age>50 years old • Neck Circumference >40cm • Gender-Male
Preoperative Assessment (Cardiovascular) • Check for HPT • Assess for IHD (angina/Exertional dyspnea) • Assess symptoms and sign of cardiac failure • Effort tolerance (walk to the length of the ward) • Ability to lie flat/supine • Position of sleeping • Orthopnea/ Paroxysmal Nocturnal Dyspnea
Airway Assessment • Head and Neck flexion/Extension/lateral rotation (cervical limit) • Jaw mobility/Mouth opening • Oropharynx (excessive palatal and pharnygeal soft tissue) and dentition • Patency of nostril • Previous anaesthetic experiences • Mallampati score • Neck Circumference (>17.5in/40cm) • The single biggest predictor of problematic intubation in morbidly obese patients • 40 cm neck circumference = 5% probability of a problematic intubation • 60 cm neck circumference = 35% probability of a problematic intubation • Fat face & cheeks, large breast, short neck, large tongue, high anterior larynx
Airway assessment • Role of imaging if time permit - soft tissue xray/CT scans with consultation with Otolaryngologist for direct/indirect laryngoscopy • Consider and discuss re: Awake fibre optic intubation with patient Anticipate difficult ventilation/intubation
Investigation • Tailored to individual (comorbid/type/urgency of surgery) • FBC, Electrolytes, Renal, Liver function, Blood Glucose (Basic) • Arterial Blood Gas (maybe useful) in suspected respiratory comorbid (OSA, OHS, pulmonary disease)-provide guide to weaning and expecting postoperative respiratory support • Preoperative ECG (to exclude significant rhythm disturbances, corpulmonale, guide for further extensive study
Echocardiography • Transthoracic may be difficult (poor window) • May estimate systolic and diastolic function, chamber dimension • CXR - assess CTR, evidence of cardiac failure • Pulmonary function test – may reveal restrictive pattern but not done on all patients • Exercise ECG testing (stress test)- impracticle
Pharmacokinetics of anaestheticagenst • Calculation of appropriate dose may be difficult • Should based Actual Body Weight or Ideal Body Weight? • Most PF of anaesthetic agents influenced by mass of adipose tissue, producing prolonged and less predictable effect • Volume of central compartment is largely unchanged • BUT dosages of lipophilic drugs need to be adjusted due to changes in Vd • Less fat soluble drugs show little or no change in Vd • lean body mass/ IBW + 20% • Exception: Scolene based on ABW, sames as
ObesityEffects on Drug Distribution • Volume of Distribution in Obese patients is affected by: • Reduced total body water • Increased total body fat • Increased lean body mass • Altered protein binding • Increased blood volume • Increased cardiac output
ObesityEffects on Drug Elimination • Hepatic clearance is not usually effected • Renal clearance of drugs is increased in obesity because of increased renal blood flow and glomerular filtration rate
ObesityHow does it effect drug dosing? • Highly Lipophilic • Barbiturates and benzodiazepines have an increased volume of distribution • Less Lipophilic • Little or no change in volume of distribution with obesity • Increased blood volume in the obese patient decreases the plasma concentrations of rapidly injected intravenous drugs. • Fat has poor blood flow and doses calculated on actual body weight could lead to excessive plasma concentrations. * Review Barash et al table 47-5*
ObesityInduction of General Anesthesia • Adequate preoxygenation • Rapid desaturation because of increased oxygen consumption and decreased FRC • Positive pressure ventilation during preoxygenation decreases atelectasis formation and improves oxygenation • Patient position • The head-up (reverse tredelenburg) position provides the longest safe apnea period during induction of anesthesia
ObesityPatient positioning • Supine • Causes ventilatory impairment and inferior vena cava and aortic compression • Trendelenburg • Further worsens FRC and should be avoided • Reverse tredelenburg • Increased compliance results in lower airway pressures • Prone • Detrimental effects on lung compliance, ventilation and arterial oxygenation • Increased intra-abdominal pressure worsens IVC and aortic compression and further decreases FRC
Obesity Ventilating the obese patient • Tidal volumes greater than 13 ml/kg offer no added advantage • Increasing tidal volume beyond 13 ml/kg increases PIP without improving arterial oxygen tension • Positive end-expiratory pressure (PEEP) is the only ventilatory parameter that has consistently been shown to improve respiratory function in obese patients • PEEP may reduce venous return and cardiac output