Download

1 / 62
650 likes | 1.05k Views
Cut Wrist & Flexor tendon injury. Ramy El Nakeeb, MD. Orthopaedic Department Damanhour Medical institute. ANATOMY. FDS FDP FPL Lumbricals origin from radial side of FDP. FDS divides and passes around the FDP tendon, the two portions of the FDS reunite at “Camper’s Chiasma ”.

E N D
Cut Wrist & Flexor tendon injury Ramy El Nakeeb, MD. Orthopaedic Department Damanhour Medical institute
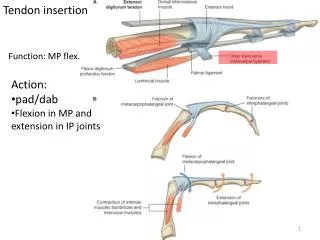
ANATOMY • FDS • FDP • FPL • Lumbricals origin from radial side of FDP
FDS divides and passes around the FDP tendon, the two portions of the FDS reunite at “Camper’s Chiasma” CAMPER’s CHIASMA
PULLEYS Preserve A2 and A4 pulley to prevent bowstringing. NOTE: There is a mistake in this diagram: The C1 pulley is DISTAL to the A2 pulley!
TENDON EXCURSION • 9 cm of flexor tendon excursion with wrist and digital flexion • only 2.5 cm of excursion is required for full digital flexion with the wrist stabilized in neutral position
BLOOD SUPPLY • Segmental branches of digital arteries which enter the tendon through: • vincula • osseous insertions • Synovial fluid diffusion
The goals of the surgical treatment is to achieve a primary tendon repair of sufficient tensile strength to allow application of a postoperative mobilization and rehabilitation protocol.
It is well-known by hand surgeons that the catastrophic potential of a volar wrist laceration can result in a functionless extremity. Tendon repair can be expected to heal and maintain individual gliding function when primary repair is coupled with early and aggressive occupational therapy.
Tendon Injury in Cut Wrist • Zone of injury • Complications • Management • In the Emergency Room • First aid • Calm the patient • Examination • Surgical repair • Rehabilitation • Cut wrist in a child
Tendon Injury in Cut Wrist • Zone of injury • Complications • Management • In the Emergency Room • First aid • Calm the patient • Examination • Surgical repair • Rehabilitation • Cut wrist in a child
Cut wrist injuries were defined as lacerations occurring between the distal wrist crease and the flexor musculotendinous junctions. It may involve as many as 16 different structures, including 12 tendons, 2 nerves, and 2 arteries.
Tendon Injury in Cut Wrist • Zone of injury • Complications • Management • In the Emergency Room • First aid • Calm the patient • Examination • Surgical repair • Rehabilitation • Cut wrist in a child
Adhesion formation • In many instances, it is unrealistic to expect a tendon to heal without any adhesions, some loose adhesions may develop after surgery even with exercise. • Adhesions influence tendon movement depending on their density. • loose adhesions arise from the subcutaneous tissue • adhesions of moderate density • dense adhesions arise from the bony floor or volar plates • A fourth type are adhesions between the repaired tendons.
Repair rupture • Among all the consequences of flexor tendon surgery, repair ruptures are of prime concern to hand surgeons, because they require secondary operations. The following factors may trigger the ruptures: Overload of the repaired tendons Tendon edema or bulky tendons Triggering in pulleys or edges of opened sheath
Joint stiffness • Clean-cut flexor tendon injuries themselves, however, usually do no trauma to finger joint structures. It is the postoperative protective finger position that causes joint contracture.
Nerve injury • May lead to insenate hand • Loss of intrensic function
Vascular injury • Cold intolerance • ischemia
Tendon Injury in Cut Wrist • Zone of injury • Complications • Management • In the Emergency Room • First aid • Calm the patient • Examination • Surgical repair • Rehabilitation • Cut wrist in a child
First aid: Cut wrist • Tendon injury • Nerve injury • Vascular injury Emergency????
Vascular injury Pleeeease Do not clamp & No stitches ischemia bleeding • Removal of tourniquet • elevation of the hand as high above the heart as possible. • packing of the wound and direct pressure Did not stop Bleeding from a partially severed vessel
Cut wrist • Why not directly into the OR ? 1. you can miss something 2. you can avoid operating and transfer the case if no proper facilities or expertise are available. 3. A superficial wound ????
Examination • What to search for in your examination ? • Diagnosis of tendon injury
TENODESIS EFFECT • Passive extension of the wrist does not produce the normal “tenodesis” flexion of the fingers if flexors are injured
FDP RUPTURE • No active DIP motion (present passive DIP motion)
Tendon Injury in Cut Wrist • Zone of injury • Complications • Management • In the Emergency Room • First aid • Calm the patient • Examination • Surgical repair • Rehabilitation • Cut wrist in a child
I must have with me: • Basic instruments.
Identification and tagging • 1.Distal structures • 2. Proximal structures should be identified from deep to superficial and tagged……..N.B. Follow the Hematoma • 3. FDS 3 4 5 2
numerous studies have demonstrated the superiority of the four-strand core suture overthe two-strand core suture and the greater strengths achieved with six- and eight-strandcore suture techniques. • The limiting factor to more widespread use of modern multistrand suture techniques remains the surgeon’s ability toperform the repair using atraumatic techniquesuch that trauma to the tendon stumps and the circumferential visceral epitenon is minimized.
How to choose which kind of repair ?? the epitendinous suture
2 Suture material: non absorbable Suture caliber :4-0 3-0, (the mode of failure was affected by the configuration and the caliber of suture used) The needle
Nerve Repair The purpose of performing a nerve suture is to align, as accurately as possible, the corresponding fascicular components of the proximal and distal nerve segments. The evolution of surgical techniques has passed through many stages. One important step was the introduction of the operating microscope, which made it possible to identify and manipulate nerve structures with improved accuracy.
Nerve injury crushing Clean cut Do not clamp Apparent Not apparent Direct sutures Trim+ direct repair, if under tension primary grafting Direct sutures will give bad results
Tendon Injury in Cut Wrist • Zone of injury • Complications • Management • In the Emergency Room • First aid • Calm the patient • Examination • Surgical repair • Rehabilitation • Cut wrist in a child