Download
1 / 33
350 likes | 605 Views
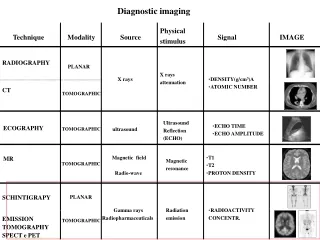
Thoraco-Lumbar Radiography. Moritz Haager March 4, 2004. Anatomy. Thoracic Spine. Lumbar Spine. Determinants of Stability. T & L spines are more stable than C-spine Strong ligaments Stabilization by ribs Bigger intervertebral discs Larger facet joints Less mobility

E N D
Thoraco-LumbarRadiography Moritz Haager March 4, 2004
Determinants of Stability • T & L spines are more stable than C-spine • Strong ligaments • Stabilization by ribs • Bigger intervertebral discs • Larger facet joints • Less mobility • Fractures & dislocations tend to occur where curvature changes • T11-12 (thoracolumbar junction) • L5-S1 (lumbosacral junction)
Mechanisms of Injury • Hyperflexion +/- rotation • Commonest • Usually see anterior wedge #’s or Chance # • Shearing • Ant or post translation • Hyperextension • Axial loading • Compression or burst #’s
3 Column Model • Anterior column • Ant longitudinal lig • Ant annulus fibrosis • Ant vertebral body • Middle column • Post longitudinal lig • Post annulus fibrosis • Post vertebral body • Posterior column • Spinous processes • Transverse processes • Lamina • Facet joints • Pedicles • Post ligamentous complex • 2 or more columns disrupted = unstable • Most disruption of middle columns are unstable
Stable or Unstable? • Radiographic findings suggestive of instability • Vertebral body collapse w/ widening of pedicles • > 33% canal compromise on CT • > 2.5 mm translation b/w vertebral bodies in any plane • Bilateral facet dislocation • Abnormal widening b/w spinous processes or lamina and > 50% anterior collapse of vertebral body
Stable or Unstable? • Checklist for Instability • Anterior elements disrupted 2 pts • Posterior elements disrupted 2 pts • Saggital plane translation > 2.5 mm 2 pts • Saggital plane rotation > 5o 2 pts • Spinal cord or cauda equina damage 2 pts • Disruption of costovertebral articulations 1 pt • Dangerous loading anticipated 2 pts • 5 or more pts unstable until healed or surgically stabilized
Stable or Unstable? • Risk of neurologic injury increases with • > 35% canal narrowing at T11-12 • > 45% canal narrowing at L1 • > 55% canal narrowing at L2 & below
Approach to T & L Spines • A – adequacy & alignment • All vertebrae need to be visible • Ant & post longitudinal lines • Facet joints should lie on smooth curve • Normal kyphosis & lordosis • All spinous processes should lie in straight line • B – bones • Trace cortical margins of each vertebrae • Difference b/w ant & post body ht < 2 mm • Progressive increase in vertebral body ht moving down spine • Wink sign & interpedicular distance • Don’t forget to look at transverse processes
Approach to T & L Spines • C – cartilage • Progressive increase in disc space moving down spine (except L5-S1) • Facet joint alignment • S –soft tissue • Look at paraspinal stripe and prevertebral space
Case 1 • 38 yo female brought to ED after being backed over by car driven by boyfriend • Intoxicated; c/o back pain & demonstrating the remarkable versatility of the F-word
Transverse process fractures of L2-4 Significance of transverse process fractures is not the fractures in and of themselves but rather the high incidence of associated serious intraabdominal injury (~20%)
Case 2 • 46 yo male presents to ED after falling 12 feet off ladder while putting up Christmas lights c/o back pain
Anterolisthesis Of L4 on L5
CT demonstrates chronic anterolisthesis with no intrusion into spinal canal
Case 3 • 50 yo male again 10-12 foot fall off ladder while putting up Christmas lights (dangerous hobby)
Mild ant wedging of T3 & T4
Mild ant wedging of T3 & T4
Case 4 • 21 yo belted passenger in rollover single vehicle MVA at highway speed
Widened paraspinal line suggesting hematoma Laterally displaced T5 pedicle Anterior wedging of T4 & T5 w/ loss of 30-40% of body ht
Case 5 • 29 yo driver offroading in pick-up truck – rolls it at speed • Not belted, ejected from vehicle and trapped underneath for 3 hrs
Paramediastinal soft tissue density & widening Suggestive of compression fractures
Case 6 • 22 yo male single vehicle rollover. Not restrained – ejected through windshield at highway speeds
Posterior displacement Involvement of pedicles & laminar arch Comminution & anterior wedging of L2 w/ 50% loss of body Ht
CT demonstrates severe burst # w/ horizontal plane extending posteriorly through pedicles and transverse processes in keeping w/ a CHANCE fracture
Case 7 • 58 yo roofer presents to ED unconscious after plunging 12 feet onto concrete through skylight
Schmorl’s node Compression fracture of L3 w/ no obvious post element involvement