Download

1 / 37
370 likes | 381 Views
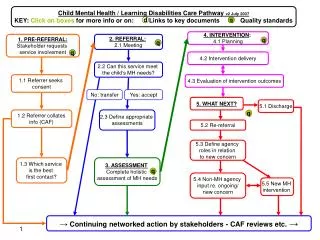
Screening, Brief Intervention & Referral to Treatment (SBIRT) An Overview. Bonnie McRee, PhD, MPH Department of Community Medicine & Health Care University of Connecticut School of Medicine mcree@up.uchc.edu. University of Connecticut Health Center Partners.

E N D
Screening, Brief Intervention & Referral to Treatment (SBIRT) An Overview Bonnie McRee, PhD, MPH Department of Community Medicine & Health Care University of Connecticut School of Medicine mcree@up.uchc.edu
University of Connecticut Health Center Partners Provide training and program evaluation for the CT SBIRT initiative Over 25 years of conducting screening and brief intervention clinical trials, implementation programs and evaluation efforts Participate in WHO working groups to develop screening instruments and brief intervention protocols for at-risk substance use
Program Rationale Use of tobacco, alcohol and other drugs is a leading cause of preventable death in the U.S. Most affected individuals receive no treatment Early identification and intervention works The CT SBIRT Program is putting early intervention into practice
Actual Causes of Death in the United States • Modifiable risk factors are the leading causes of mortality in the U.S. • Tobacco use (18%) • Poor diet and physical inactivity (17%) • Alcohol consumption (3.5%) • Other actual causes: microbial agents, toxic agents, motor vehicle crashes, firearms incidents, sexual behaviors and illicit use of drugs. Mokdad, Marks, Stroup & Gerberding. (2004); JAMA, 291, 1238-1245.
National Survey on Drug Use and Health (NSDUH, 2010) • Current use • Cigarettes: 58 million (23%) • Binge drinking: 58 million (23%) • Marijuana: 17 million (7%) • Prescription drugs (non-medical): 7 million (3%) • Abuse or dependence: 22 million (9%) • Received treatment: 2 million
Dependent At Risk Lower Risk Abstainers Alcohol Use and Related Problems
Referral to intensive treatment Brief Intervention Brief Treatment A B S T A I N USE AT-RISKUSE ABUSE DEP Use Consequences* *Loss of control, preoccupation, compulsivity, physical dependence Edited from slide presentation by Katie McQueen, Texas InSight Program + - + -/+ + + + ++ - -
At-Risk Drinking Per OccasionPer Week Men >4 drinks >14 drinksWomen >3 drinks >7 drinks
Substance Abuse - DSM IV Maladaptive pattern of use leading to impairment as manifested by at least one: • Recurrent use resulting in failure to fulfill role obligations at work, school or home • Recurrent use in physically hazardous situations • Recurrent substance-related legal problems • Continued use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects And does not meet criteria for DEPENDENCE
Substance Dependence - DSM IV Maladaptive pattern of use leading to impairment as manifested by three or more: • Tolerance • Withdrawal • Using more and/or using for longer times • A desire or repeated attempts to cut down • Lots of time using or recovering • Reduced activities: social, work, recreation • Recurrent use despite physical and psychological problems
What is SBIRT? • Screening is method for identifying someone at risk for a condition • Validated assessments include ASSIST, AUDIT, DAST, FTND • Screening score provides an assessment of patients’ risk levels (lower, moderate, high) • Health Educator conducts screening in general medical, dental or other departments
What is SBIRT? • Brief Intervention is low-intensity, short-duration counseling for those who screen positive • Utilizes a motivational interviewing approach • Includes feedback of risks and advice to change • Health Educator conducts immediately following screening or after the patient’s medical or dental exam
What is SBIRT? • Referral to Treatment facilitates access to care for individuals with more serious signs of substance use disorders • Health Educator refers patient to substance abuse therapist within behavioral health dept. • Diagnostic assessment • Brief Treatment (MET, CBT) • More intensive treatment
BI Example Dentist and patient Track 3 9:57-13:23
Broadening the Base of Treatment • Early intervention vs. traditional treatment • At-risk use vs. dependence • Public health vs. individual perspective • Risk factors vs. disease conditions
Early Detection/Intervention Trend • No real effort prior to 1980’s to target risky behaviors • Smoking before lung cancer developed • At-risk alcohol use before liver cirrhosis • Progress in preventive services for early detection of diseases increased popularity of early interventions • Cervical cancer and hypertension screening • “Broadening the base of treatment” by screening for behavioral risk factors in medical patients likely to develop any number of preventable medical conditions occurred.
SBIRT Research Base • Since 1980, several hundred empirical studies on screening, brief intervention, referral and integration of SBIRT into health care settings • Over 25 screening tests developed and validated • Scores of randomized controlled trials of brief intervention in a wide range of countries • 15+ integrative literature reviews • A growing literature on provider training, program implementation, and new applications
Summary of Brief Intervention Evidence With At-risk Drinkers • Patients receiving brief interventions reduced average number of drinks/week by 13% to 34% compared to controls • Proportion of participants in intervention condition drinking at moderate or safe levels was 10% to 19% greater than controls • Negative findings reported in some ED studies (i.e., no reduction in alcohol use) but decreased the odds by half of experiencing alcohol-related injuries compared to controls • (Bien et al., 1993; Havard et al., 2008; Kaner et al., 2009; Nilsen et al., 2008; Whitlock, et al, 2004)
Health and Related Outcomes • Quality of life measures • Improved quality of life related to alcohol problems for those who decreased consumption by 20% or more • Long-term health outcomes • Fewer hospital days at 48 months by intervention group (429 vs. 664 days; p<.05) (Fleming, et al, 2002) • Significantly greater reductions in alcohol use by intervention group over 48 months • Malmo Screening and Intervention Study • Lower total mortality (24/100,000 person years) than controls (30/100,000; p<.02), and significantly reduced alcohol-related mortality after 3 and 21 years (Berglund, et al, 2000)
Brief Intervention Evidence for Other Substances • Significant literature for brief smoking cessation counseling (Fiore et al., 2008) • MTP Research Group (2004) – cannabis (US) • Copeland et al. (2001) - cannabis (Australia) • Heather et al. (2004) – benzodiazepines (UK) • McCambridge and Strang (2004) - cigarettes and cannabis (UK) • Bernstein et al (2005) - cocaine and heroin (US) • Madras et al. (2008) – 4 categories of drugs • WHO ASSIST Working Group (in press) – 4 categories of drugs (Brazil, Australia, India, US).
Research to Practice Gap • Large research base supporting the efficacy of SBIRT services for general medical patients, especially for interventions targeting at-risk alcohol and tobacco use • Growing evidence for efficacy of SBIRT for other substance use • However, technology from SBIRT clinical trials has not being widely adopted by medical professionals in the field
Is it Time to Translate a Public Health Approach to SBIRT? • Prerequisites for public health approach • Is the problem prevalent? • Is there an adequate definition of the problem and operational criteria for diagnoses? • Are screening tests available, brief, simple to administer and valid in different cultural settings? • Are there effective intervention and treatment methods available?
SAMHSA’s SBIRT Implementation Initiative • SBIRT grant program initiated in 2003 with cooperative agreements to 7grantees (Cohort 1) • Coordinated effort to promote widespread adoption of SBIRT by • Expanding the grantee’s continuum of care to include SBIRT in non-traditional SA treatment settings • Supporting clinically appropriate treatment services for non-dependent substance users • Improving linkages among community agencies that are implementing SBIRT and SA treatment agencies
Current SBIRT Programs • 24 state/territory/tribal organization grantees • 4 cohorts of grantees • Expand grantees’ continuum of substance abuse care to medical and other community settings • 12 campus-based programs at colleges and universities • Combat underage drinking and promote innovative SBIRT practices in the context of student health care • 17 medical residency cooperative agreements • Promote the adoption of SBIRT among primary care and specialty medical residents
Implementation of Evidence-based Practices What is known (evidence base) is not routinely adopted in practice to improve health care What is implemented is typically not used with fidelity and thus may not improve patient outcomes What is implemented disappears with time, staff turnover and decreased funding Very little experimental evidence regarding implementation outcomes (e.g., fidelity, adoption, model migration, integration, sustainability)
SAMHSA’s SBIRT Cross-site Evaluation Team • RTI International • JBS International, Inc. • University of Connecticut Health Center • The Avisa Group
SBIRT Cohort 1 Grantees and Settings Grantees Settings Hospitals Emergency Departments Trauma Centers Community health centers Schools and student assistance programs • California • Cook Inlet Tribal Council • Illinois • New Mexico • Pennsylvania • Texas • Washington
Process Evaluation of Cohort I Grantees Describe how different grantee initiatives have implemented the general SBIRT concept Organize performance data so that implementation models can be compared within settings across different SBIRT components Provide deeper insights into implementation obstacles and real-world issues that challenge SBIRT
SBIRT Model Matrix Conceptualized by Babor & McRee, 2006
SBIRT Cohort I Performance A complex public health program was implemented in approximately 118 diverse sites Cohort I grantees succeeded in reaching their target populations: By February, 2009, more than 750,000 patients were screened, many of whom would otherwise not have been served. 45% of those who screen positive report using an illicit drug Patients who screen positive for tobacco or at-risk alcohol use have a high probability of screening positive for other drug use
SBIRT Cohort I Performance As a public health approach, screening for illicit drug use in medical settings proved to be acceptable and efficient when combined with alcohol and tobacco protocols Illicit drug use by BT and RT patients was almost double that for the BI group; more than 1 in 10 RT patients reported injection drug use Referred patients reported experiencing stress, activity loss, and emotional problems as a result of substance use, and a variety of ancillary problems Grantees have initiated a variety of strategies (including the use of BT) to refer and engage patients in specialty treatment
Lessons Learned:Important Facilitators Leadership (“champions”) and buy-in at all organizational levels Integration of SBIRT Health Educators within the host medical setting Staff acceptance of the SBIRT model (non-dependent users, MI, behavioral health within a medical setting) Strong collaborative partnerships among agencies that are developed and nurtured over time Effective use of technology Strong training and performance monitoring protocols incorporating feedback loops
Lessons Learned:Service Delivery Models (1) Programs often require adaptations (e.g., adoption of a pre-screen) to meet program goals and function effectively within the specific real-world settings in which they are embedded. The Contracted Specialist service delivery model has worked well for the CSAT SBIRT grantees, often addressing implementation barriers. Evidence-based practice is enhanced by appropriate training, and by sustained supervision, monitoring, and feedback. Patients who screen positive often have ancillary physical, medical, and mental health issues that require consideration in the treatment referral process.
Lessons Learned:Service Delivery Models (2) Brief treatment can serve a variety of important functions within the continuum of care, providing: An appropriate level of care for non-dependent alcohol and drug users who require more than brief intervention; An acceptable, evidence-based treatment alternative for patients who are unable or unwilling to enter conventional specialty programs; A bridge to specialty services that increases motivation for change and facilitates treatment engagement Co-location of BT services within the host medical setting improves access to care and treatment initiation
Lessons Learned:Efficiency and Viability (1) SBIRT programs in large-volume settings are particularly effective from a public health perspective: They serve captive populations with high proportions of individuals at-risk They provide an efficient use of resources
Lessons Learned: Sustainability Most grantees have sustained SBIRT services at some original performance sites, although often at reduced capacity Smaller, lower-volume SBIRT programs have been harder to sustain than high-volume, urban hospital sites Sustainability efforts by grantees have included a variety of strategies: Accessing new grants from other agencies and provider entities Placing continuation funding in pending state legislation Screening for substance use within the context of a broader behavioral health screening protocol Altering the mix of services offered
For Further Information, Please Contact Bonnie McRee Department of Community Medicine & Health Care University of Connecticut School of Medicine mcree@up.uchc.edu 860-679-5485