Download
1 / 27
270 likes | 271 Views
ELFT Training Packages for Primary Care ‘ Introduction to Child & Adolescent Psychiatry ’ Influences on mental health development and approaches to assessment. CAMHS ELFT Graeme Lamb Clinical Director. Learning outcomes: By the end of the lecture you should.

E N D
ELFT Training Packagesfor Primary Care ‘Introduction to Child & Adolescent Psychiatry’Influences on mental health development and approaches to assessment CAMHS ELFT Graeme Lamb Clinical Director
Learning outcomes: By the end of the lecture you should • Understand the complex aetiology of childhood mental health and behavioural problems • Be able to describe the impact of different systems on the psychological development of children and young people • Understand the effect of chronic medical or developmental problems on the family unit • Understand the need to consider developmental factors when assessing a young person • Understand the principles of taking a history from a young person and their family • Understand the approach to conducting a mental state examination of a child and how to present the findings in a logical manner
Introduction: There is no health without mental health (1) • But what is mental health? • What is child mental health? • Does everyone agree? • Consider the following images • Should they be seen/treated by a child psychiatrist? • Are there any factors that would influence your answer? 1 Closing the gap: Priorities for essential change in mental health (2014). Department of Health
Temper Tantrums • Factors that might influence your decision • Age of child • Severity • Frequency • Impact
Hearing voices • Factors that might influence your decision • Nature of voice • Developmental age of child • Context • Impact Consider that 20 of 11-13 year olds report hearing voices (2) 2. Clinico-pathological significant of psychotic experiences in non-psychotic people: evidence from four population-based studies. I Kelleher et al 2012 BJPsych
Why learn about Child Psychiatry? • 20-30% of GP consultations involve children • 45% of medical students become GPs • Although (3) • 2-5% of children present with emotional or behavioural symptoms as the presenting feature • The rates of psychiatric disorder are much higher • 7-12 year olds: 1 in 4 • 13-16 year olds: 4 in 10 • Half of people with lifetime mental health problems had difficulties since before age 14 (4) 3. Child and adolescent mental health problems in primary care (2000). Kramer and Garralda. Advances in psychiatric treatment (6) p287-294 4. Age of onset of mental disorders: A review of recent literature (2007). Kessler et al. Current Opinion in Psychiatry. 20(4): 359-364
Definition of psychiatric disorders • Abnormalities of behaviour, emotions and relationships that impair a young person’s function • ABNORMAL is defined in relation to • child’s age and gender • developmental stage • culture • persistence • extent of disturbance • severity and frequency • IMPAIRMENT • causes suffering to child/distress to family • social restriction • impedes the child’s development • effects on others
The epidemiology of child psychiatric disorders • Data on epidemiology is needed to plan services. • Available UK data is quite out of date – updates are required • Data from the Office of National Statistics Survey in 2004 (data shown is prevalence in %) (5) Around 1 in 10 children 5. Mental health of children and young people in Great Britain (2005) ONS 6. Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP). G Baird et al. The Lancet 2006 Vol 368 p210-215
Aetiology of child psychiatric disorders MULTIFACTORIAL Consider factors involving: • Child • boys • low intelligence • difficult temperament • physical illness • developmental delay • genetic factors • Family • See following slides • Environment • peer relationship problems • social deprivation • school factors • stresses resulting from accidents
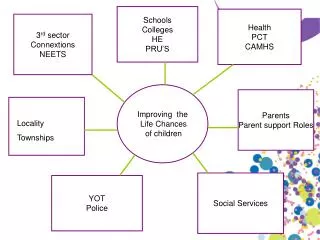
The child’s world Individual Family School & social life Social situation – neighbourhood, community Problems or disturbances at any of these levels can cause mental health difficulty
Family and culture • The whole family unit needs to be considered in the context of culture/ethnicity/religion/social factors • A young person is part of many different systems • Each of these will have an impact on the presentation but also the family’s understanding of the problem and the most helpful treatment. • Consider • Sibling relationships • Parental relationships • School/Peers • Extended family • Neighbourhood and community • Religion • Culture and Race
The Family… • Family has an important part to play in a developing young person. • Consider the following diagram, what might the impact of different family influences be? • Influences on attitudes to education • Emotional expression • Security • Management of threat • Experiences of separation and loss • Attachment relationships • Intimacy • Sense of autonomy and individuation • Law and moral values • Role of ethnicity, religion and culture
Familial Transmission • Familial transmission is not just about genetics • Genetic factors: schizophrenia, ASD, ADHD • Biological hazards: foetal alcohol syndrome • Models of behavior and attitudes: offending, eating, alcohol use • Intergenerational continuities: maternal relationship to child influenced by her relationship to her own mother • Broader social context social adversity, unemployment, isolation, few community resources, migration
Parenting/Care Factors • Abuse/Maltreatment • Physical: • Sexual • Emotional • Neglect • Poor parenting techniques • Lack of boundary setting • Illness behaviour • Factitious illness • Somatisation
Aetiology and formulation of child psychiatric disorders: • Consider whether child, family, environmental factors are: • PREDISPOSING • PRECIPITATING • PERPETUATING • WHAT IS PROTECTIVE AND AIDING RESILIENCE?
How do we assess a child? • First appointment: • First opportunity to meet child and family • Important for establishing therapeutic engagement • Setting: • Not just in clinic • Consider family home, nursery/school or other group. • Sources of information • GP • School • Community paediatrics • Social care • Practice point: Always consider the child’s physical health and any red flags (covered in other lectures)
What to look for in the history? • What do the parents see as the problem? Are there any disagreements about this? • Nature of problems (take in the same kind of detail as you would a pain history, and get good descriptions of any problem behaviours) • Behavioural problems • Emotional problems • Attention and concentration, Activity level • Developmental history • School history • Physical health • Family structure, relationships, history of illness • Interventions so far
What to look for in the child’s behaviour • What do you observe during the session? • What does the child do? • Speech • Overall level of development • Compare with appropriate developmental stages • Assessing interactions with others • Does the child seek support/proximity to the main carer? (please refer to session on attachment) • Does the child seek support or avoid any family member? • How does the child play with siblings? • What is the child playing with? • Will the child engage with you?
Mental State Examination: older child • Appearance and behaviour • Mood • Speech • Thought process and content • Perception • Cognition • Insight and Judgement • Risk • Practice point: Always see an Adolescent alone at some point during the assessment
Interplay with the child’s physical health • Is the child acutely unwell? • Does the child have a pre-existing medical problem that may be affecting their mental health and behaviour? • Are there any effects of medication or treatment? • Does the child have a developmental problem?
Interplay with the child’s development • Pregnancy and birth history • Developmental milestones • Consider the child’s physical, cognitive, social and emotional development.
Formulation and management plan • A formulation is a summary of the child’s difficulties including any developmental or physical problems with a consideration of family and cultural context. It will include if there have been any precipitating factors for example change in family circumstances/starting school. • A management plan describes what you will do for the child yourself and via other agencies. It includes treatment options, a risk management plan and a review date.
Treatment approaches in child & adolescent psychiatry Work with the network Children and families often have many agencies working with them Provide consultation and advice Work with the child Who do we work with? Work with parents/carers Work with the family Psycho-education Explanations in appropriate format for culture/learning/understanding of young person AND family Talking therapies CBT Family therapy Psychodynamic therapy Pharmacotherapy Stimulant medication Anxiety and depression antipsychotics Parent training/advice Very important for all behavioural problems Group Vs Individual Setting Normally outpatient AGE: Up to 12 – v rarely treated as inpatient AGE 12+ - if risk is too great to treat at home with parents
Summary • Assessment and treatment reflects the multifactorial aetiology of child and adolescent emotional and behavioural problems • Developmental factors must be taken into consideration when assessing any presenting feature • It is important to consider the severity and impact of any problem