Download
1 / 44
620 likes | 916 Views
Fecal Microbiota Transplantation (FMT). Bret Lashner, MD Cleveland Clinic. Early History of FMT. 4 th Century ( Ge Hong) : Oral human fecal suspension ( “ yellow soup ” ) for severe diarrheal illnesses, food poisoning

E N D
Fecal Microbiota Transplantation (FMT) Bret Lashner, MD Cleveland Clinic
Early History of FMT • 4th Century (Ge Hong): • Oral human fecal suspension (“yellow soup”) for severe diarrheal illnesses, food poisoning • 16th Century (Li Shinzen): fermented fecal solution, dry feces - treated fever, severe diarrhea, vomiting and constipation • 17th Century: Veterinary medicine • Fecal transfer for horses with diarrhea • 1958: FMT enema • Eismann, et al. 4 patients with pseudomembranous colitis • “Dramatic” response within 48 hours
Yellow Soup or Cappuccino? Cleveland Plain Dealer, October 21, 2015
Fecal transplantation in veterinary medicine since the 17th century • Transfaunation • Horses with diarrhea- infuse stool from healthy horse per rectum • Cattle - per os as rumen
Human Intestinal Microbiome • Includes bacteria, archea (single-celled prokaryotes), viruses, fungi and parasites • Only 10 of more than 50 known bacterial phyla • Bacteroidites, Firmicutes~ 90% gut microbiota • 1014 bacterial cells 10 times greater than number of human cells in our body • Diversity within phyla, vary widely between individuals Eckburg, PB et al. Science 2005:308;1635-8
Different ages and geographic populations have very different microbiomes Population Age Yatsunenko et al. 2012 Nature
The mammalian gut microbiota (Ley et al) Divisions % sequences Firmicutes 69 Bacteroidetes 17 Actinobacteria 6 Proteobacteria 5 Gemmatimonadetes 0.02 Defferibacteres 0.1 Verrucomicrobia 2.1 Lentisphaerae 0.08 Planctomycetes 0.08 *@CD Gut 1 0.2 *@CD Gut 2 0.01 Fusobacteria 0.9 Spirochaeates 0.7 Fibrobacteres 0.08 *Cyano Sister 0.15 Synergistes 0.12 Chloroflexi 0.01 *TM7 0.04 *: no cultured representatives @: novel candidate division • Firmicutes and Bacteroidetes dominate across all mammals. • Dietary influence: • Carnivores have the fewest divisions and are most enriched in Firmicutes. • Humans are typical omnivores; cluster with omnivorous primates; leaf-eating primates cluster with herbivores
Fecal Microbiota Transplantation (FMT) • Definition: Instillation of stool from a healthy person into a sick person to treat a certain disease • Rationale: A perturbed imbalance in our intestinal microbiota (dysbiosis) is associated with or causes disease and can be corrected with re-introduction of donor feces
Conditions Potentially Treatable By FMT Smits LP, et al. Gastroenterology 2013;145:946-53
C. difficile Infection (CDI) • Spore-forming, anaerobic, gram -positive • Leading cause of healthcare-associated infectious diarrhea in US • - 3 million cases per year-1996 – 2009 in U.S., rates of CDI doubled • Unadjusted fatality rate • 1.2 % (2000) 2.3% (2004) • Majority > 65 y/o • ~ 3.2 billion dollars excess cost of care Gastroenterology 2012 Nov;143(5):1179-1187
C. difficile Manifestations • Carrier state • C. difficile- associated diarrhea (CDAD) • C. difficilecolitis • Pseudomembranous colitis • Fulminant Colitis / Toxic megacolon • Atypical (e.g., sepsis, ascites) • Recurrent disease Khanna AJG 2012
Recurrent CDI • 15-20% of patients • Relapse • Re-infection • Post-CDI irritable bowel syndrome • 2ndrecurrence: 40%; 3rd recurrence 60% • Rx failure before 2003 < 10%; after 2003 ~ 20% • Relapses can continue for years • No universal Rx algorithm
Why Do We Get Recurrent CDI ? • Virulence of infection • Impaired host-response • Altered intestinal microbiome • “Dysbiosis” = decreased microbiota diversity
Host factors for recurrent CDI 1. Hookman P, Barkin, JS. World J Gastroenterol. 2009;15:1554-1580. 2. APIC. Guide to the Elimination of Clostridium difficile in Healthcare Settings. 2008. 3. Makris AT, Gelone S. J Am Med Dir Assoc. 2007;8:290-299. 4. Cohen SH, et al. Infection Control and Hospital Epidemiology. 2010;31(5):431-455. 5. Goodhand JR, et al. Ailment Pharmacol Ther. 2011;33:428-441. 6. Aseeri M, et al. Am J Gastroenterol. 2008;103:2308-2313. 7. Schaier M, et al. Nephrol Dial Transplant. 2004;19:2432-2436. • Age ≥ 65 years • Immunosuppression • recipients of organ transplants (3-11%), chemotherapy, corticosteroids, HIV, IBD, ESRD, ESLD • PPI use ≥ 3-fold • Hospitalization, long-term care facilities • After 1 week 13%, after 4 weeks > 50% colonization rate • Previous CDI
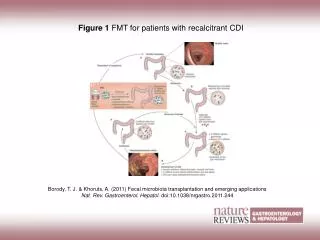
How Does FMT Work? Borody, T. J. & Khoruts, A. (2011) Nat. Rev. Gastroenterol. Hepatol.
FMT for CDAD Cammarota, J Clin Gastro 2014;48:693-702 • 20 full-text case series, 15 case reports,1 randomized controlled study through Feb 2013 • Total 536 pts with symptomatic CDAD • 467 (87%) experienced resolution of diarrhea after FMT • Diarrhea resolution rates varied according to the site of infusion: • 81% in the stomach; 86% in the duodenum/jejunum; 93% in the cecum/ascending colon; 84% in the distal colon. • No severe adverse events were reported with the procedure.
Included patients: • Median number of recurrences 3 (1-9) • Cure rate donor feces 94% • Cure rate vancomycin 23-31% 13 15 Trial stopped early - unethical to continue Van Nood N et. al. NEJM 2013;368:2145
Protocol for FMT in Recurrent CDI • Insurance Approval:$4,300. • IRB-Approved informed consent • Choose donor • Spouse/partner • 1st degree relative • Household contact • Donor exclusions • Antibiotic use within 3 months • Diarrhea, constipation, IBS, IBD, colorectal cancer, immunocompromised, anti-neoplastic drugs, high-risk behaviors • Testing • Donor Stool: culture for enteric pathogens, O&P, C. difficile • Donor and Recipient Blood: Hepatitis remote panel, syphilis, HIV, HTLV Brandt LJ ACG Meeting Oct. 2012
Protocol for FMT in Recurrent CDI • Donor • Gentle laxative (e.g. MOM) evening before FMT • Freshly passed stool • Mixed with 500mL non-bacteriostatic water/saline • Filtered • Used within 6-8 hours • Recipient • D/C antibiotics 5 days prior to procedure • Large volume bowel prep evening before FMT • Loperamide before procedure • Instill up to 500mL in the right colon Brandt LJ ACG Meeting Oct. 2012
Protocol for FMT in Recurrent CDI • Stool Transplant • Donor stool suspension with non-bacteriostatic water • Filtered • 60cc catheter tip syringe • Volume of ~ 300 mL instilled into ascending colon • Patient to hold stool for 4-6 hours Brandt LJ AJG 2012
Cleveland Clinic Outcomes • N > 150 • Average age: 63 • Indication: C difficile • 96% success in eradicating C difficile • 1 repeat FMT successful • 16 with repeat C difficiletesting - neg
Follow-up Survey Brandt LJ, et al. Am J Gastroenterol 2012:108:177-85 • 77 patients > 3 months after FMT • Duration of illness: 11 months • Symptomatic response after FMT • < 3 days in 74% • Primary cure rate: 91% • Secondary cure rate: 98.7% • 97% of patients would have another FMT for recurrent CDI • 58% would chose FMT as their preferred Rx
Cost-Effectivenes FMT • Decision analytic model comparing 4 strategies for 1st episode recurrent CDI • Metronidazole • Vancomycin • Fidaxomicin • FMT-colonoscopy • FMT most cost-effective strategy with incremental cost-effectiveness ratio of $17,016 vs Vancomycin • More cost effective than Fidaxomicin and metronidazole because of higher cost and/or lower efficacy of medications • FMT colonoscopy most cost-effective strategy with cure rate 96.4% Konijeti GG, et al. Clin Infect Dis 2014;58:1507-14 ACG 2013
Conditions Potentially Treatable By FMT Smits LP, et al. Gastroenterology 2013;145:946-53
Why don’t we alldevelop IBD when exposed to aggressive gut bacteria? Normal colon Ulcerative colitis
Fut2 Sartor, Gastroenterology 2010 Sartor RB Gastroenterology 2010
Microbiome in prevention of inflammation • Microbiotaaltered in IBD: • Decreased diversity and bacterial load: • Bacteroides • Induce T-regs and cytokines • Firmicutes • Induce T-regs and reduce inflammation in DSS induced colitis in mice • SCFA production: Butyrate-immunoregulatoryproperties Mann EA, Saeed SA. Curr Opin Gastroenterol 2011;28:24–9 Kamada Nature Reviews 2013
FMT in patients with active Ulcerative Colitis • UC pts, randomized to 50 mL retention enema, anonymous donor, • 1x/wk for 6 weeks vs placebo enema • Pancolitis - more common in transplant group • Primary outcome - remission with Mayo score of < 2; and an endoscopic Mayo score of 0, week 7. • Secondary outcome - change in QOL, assessed with the IBDQ • Trial stopped early for futility. • Stool from patients receiving FMT had greater microbial diversity than at baseline Moayyedi, P, Gastroenterology 2015: 149:102-9
Taxonomic profiles of donors used in the trial. **Donor microflora matters ** Moayyedi. P. et al. Gastroenterology, 2015 .
FMT for IBD Altered microbiome in IBD, so FMT could be useful FMT in IBD patients with recurrent C difficile is likely to be beneficial, especially if the C difficileis associated with disease flare FMT in IBD patients without C difficilehas not been shown to be helpful, possibly related to diversity of donor microflora
Atherosclerosis and Fecal Dysbiosis Mechanistic link between atherosclerosis and intestinal microbial metabolism of dietary nutrients to produce trimethylamine N-oxide (TMAO) Specific dietary nutrients – choline, phosphatidyl choline, and carnitine – eggs, liver, meat Atherosclerosis-prone strain of mice were given FMT from low TMAO producing strain Choline-rich diet led to lower atherosclerotic plaques and lower TMAO Gregory JC, et al. J Biol Chem 2015;290:5647-60
Gut microbiota-dependent metabolism of dietary phosphatidylcholine in atherosclerosis ZN Wang et al. Nature472, 57-63(2011)
Dietary/ microbial interactions impact intestinal, hepatic and vascular inflammation J Goldsmith and RB Sartor J. Gastroenterology 2014
Perfect Donor Lean No chronic diseases No infectious disease No predisposion to diabetes, or other chronic diseases like NAFLD, MS, IBD, or chronic fatigue syndrome Low TMAO-producing foods
FMT and the FDA: Existing Regulatory Framework Drug and Biologic IND requirement “Enforcement discretion” C difficileonly Source: U.S. Food & Drug Administration, www.fda.gov/AboutFDA/Transparency/Basics/ucm361441.htm
Dilemmas For regulatory agencies For patients For clinicians and clinical researchers For healthcare organizations Source: Wikipedia, https://en.wikipedia.org/wiki/List_of_The_Thinker_sculptures#/media/File:Cleveland_Museum_of_Art_-_damaged_Thinker.jpg
Capsules for FMT Youngster I, et al. JAMA 2014;312:1772-8 20 patients, open-label, relapsing C difficile *****Healthy donor volunteers***** 15 capsules on 2 consecutive days Resolution of diarrhea – 70% 4/6 non-responders responded to second FMT Overall response rate 90% No adverse events
OpenBiome No IND Donor testing: 3% of prospective donors pass testing, retested every 60 days www.openbiome.org
OpenBiome • Recommendations: • PPI • Informed Consent • Direct observation of capsules • Cost • $385 – 30mL upper GI or 250mL lower GI • $535 – 30 capsules www.openbiome.org
FMT is being conducted under an enforcement discretion from FDA—as described in a Guidance issued in 2013, followed by two Draft Guidances issued in 2014 and 2016, respectively. • The draft guidances are not enforceable, but they do reflect FDA’s current opinion on the topic, and in this case it is pretty clear they would want an IND for using capsules from OpenBiome. • The changes from 2013 to 2016 have added progressively more language circumscribing third-party specimen use without an IND, while encouraging providers to obtain and bank specimens obtained and screened under their (or their colleagues’) supervision without an IND. • OpenBiome has made it clear that since the draft guidances are not enforceable, they will not obtain an IND. • You can see that this puts us in a difficult position from a regulatory standpoint. position, from a regulatory standpoint.
The Do-It-Yourself Approach Source: “Fecal Transplant at Home — DIY Instructions,” The Power of Poop, http://thepowerofpoop.com/epatients/fecal-transplant-instructions/
and Fecal Microbiota Transplantation