Download
1 / 23
230 likes | 764 Views
Fibrous dysplasia with pathological fracture of proximal femur in a 25 year old lady. Dr N K Sinha & Dr Rajaram Pai [ Manipal campus], Melaka- Manipal Medical College Malaysia. Case history & clinical examination. A 25 year old lady sustained a trivial fall at home

E N D
Fibrous dysplasia with pathological fracture of proximal femur in a 25 year old lady Dr N K Sinha & Dr Rajaram Pai [Manipal campus], Melaka-Manipal Medical College Malaysia
Case history & clinical examination • A 25 year old lady sustained a trivial fall at home • Unable to walk after the fall • There was acute pain,swelling, deformity and abnormal mobility in upper part of her right thigh
When asked further, the patient gave a history of shorter right lower limb and restriction of right hip abduction since long
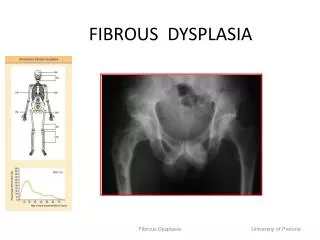
Xray AP pelvis with both hips : Pathological fracture right hip with coxavara
The femur was bent laterally Cortex was thinned and expanded Neck shaft angle was reduced Proximal femur was having a ground-glass appearance Traction AP view both hips showed
Fractureside Normal side
Skeletal survey of other bones did not reveal affection of other bones Blood investigations were within normal limits Workup
Provisional diagnosis Monostotic fibrous dysplasia with pathological subtrochantric fracture right femur
Operative procedure • Laterally based wedge was resected from distal fragment • Medullary canal was reamed • Internal fixation was done with 135º dynamic hip screw • Concellousbone graft was harvested from contralateral iliac crest - packed at fracture site and medullary canal to promote union
Operative steps Lateral based bone wedge excision Sent for biopsy Wedge closure by abduction 3 1 2
Post op day 1 135º Bone graft Post operative xray
23 weeks post op : Union & leg length restoration
Discussion • Fibrous dysplasia is a developmental disorder • There is replacement of bony structure by relatively avascular fibrous tissue within which thin trabacular bone is scattered
Skeletal affection 70 % monostotic 20% polyostotic 2-3% have associated endocrinopathy that manifests as pricocious sexual development, cafe-au-lait spots (Albright’s syndrome)
Monostotic fibrous dysplasia affects rib, femur, tibia gnathic bone, calvarium, humerus Polyostotic fibrous dysplasia affects skull, facial bones, pelvis , spine and shoulder girdle Polyostotic fibrous dysplasia maybe unilateral/ bilateral Does not affect the epiphysis Diaphysis and metaphysis are affected
Gross pathology Affected bone is irregular and bent Cortex is thin and expanded The fibrous tissue appears reddish gray/gray Feels like a fine sand paper Pathological fracture might occur but does not displace because of fibrous tissue. The femur may have outward bowing and varus deformity at neck that produces shephard’s crook deformity
Microscopy Microscopic areas of woven bone scattered in cellualar fibrous tissue Giants cells may be seen at the areas of hemosiderin deposits Cartilage is seen at the areas of cystic degeneration
Small single lesion may be asymptomatic Disease starts in childhood (before 10 years) and may progress till puberty Incidentally discovered on x-ray Bending deformity may develop in weight bearing bone followed by pathological fracture Affection of skull may cause asymmetry, cranial nerve involvement
Blood investigations are normal in most of the cases X-ray shows a radiolucent ‘cystic’ area in the metaphysis or shaft giving a hazy or ground glass appearance Sometimes there are cystic multilocular lesions causing scalloped endosteal erosion and osseous expansion Investigation
It can progress rapidly or slowly causing deformity, pain or fractures Malignant changes are 5-10 % in polyostotic lesion Majority of pathological fractures unite with treatment Natural history
It has a strong tendency to recur Large cystic lesion may bleed profusely during surgery Points to consider during surgery
Reference Apley’s System of Orthopaedics and Fractures,8thedition,Oxford university press inc.,New York