Download
1 / 58
590 likes | 974 Views
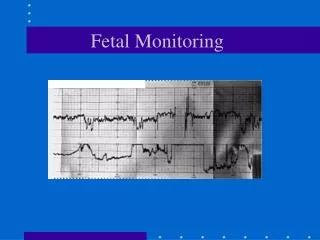
Team Communication and Fetal Heart Rate Monitoring. Texas Center for Quality & Patient Safety Michael Nix, MD. Goals. Communication strategies NICHD Fetal Heart Rate Terminology Three-Tier Fetal Heart Rate Interpretation System Resuscitative measures. Communication.

E N D
Team Communication and Fetal Heart Rate Monitoring Texas Center for Quality & Patient Safety Michael Nix, MD
Goals • Communication strategies • NICHD Fetal Heart Rate Terminology • Three-Tier Fetal Heart Rate Interpretation System • Resuscitative measures
Communication • The process by which information is transferred between individuals or teams
Components of Communication • Sender • Receiver • Message • Feedback
Communication Error Joint Commission Sentinel Event Root Causes • The leading root cause of sentinel events from 1995-2005 • In the category of maternal injury or death • Implicated in >60% of cases 1995-2004 • >80% in 2005
Focus on Getting the Message to the Recipient • JCAHO National Patient Safety Goal #2: Improve the effectiveness of communication among caregivers • One of the six main competencies of ACGME
Factors That Can Impede Effective Communication “Clinical Communication and Patient Safety” HHN Magazine, August 2006 • Different communication styles • Expert vs. novice • Hierarchy • Culture/ethnicity/language difference • Gender • Socioeconomics • History of unresolved conflict • Personality/behavior of the patient or provider • Level of respect, tone of voice, body language
Patient Care Problems Related to Poor Communication Achieving Safe and Reliable Healthcare, Leonard, et al 2004 • Providing care with incomplete or missing information • Executing poor patient handoffs with relevant clinical data not clearly communicated • Failing to share and communicate known information
Effective Communication • Complete • Concise • Clear • Timely • Allows Feedback
SBAR From Safer Healthcare (http://www.saferhealthcare.com) • Situation: Describe • What is going on with the patient? • Background: Concise and Focused • What is the key clinical background or context? • Assessment: Judgment • What is the problem? • Recommendation: What needs to happen • What do I recommend or what do I want you to do?
Incomplete information • “Decels in room 3” (Situation) • “We need you in room 3” (Recommendation) • “I need you to come assess the patient in room 3. She is having decels.” (Situation and Recommendation) • “Room 3 is having decels. The FHRT is otherwise reassuring.” (Situation and poor Assessment)
Appropriate Communication S“I’m Mike, the nurse taking care of Ms. Johnson in room 3. She is having late decels.” B“She was admitted by Dr. Not-on-call-anymore at 8 this morning for an induction at 41 weeks of gestation. She received cytotec followed by pitocin starting at 5pm. Until now, she has had a Category I tracing” A“For the last 30 minutes, she has had late decelerations with each contraction. The baseline is in the 150’s and shows minimal variability. There are no accelerations. I have stopped the pitocin, and she is contracting every 5 minutes. She was 3/thick/-3 on exam.” R“I would like you to come review the FHRT to see if you think that we should continue the induction.”
SBARR? • Response: Acknowledge and document the response of the provider • Closes the loop of communication
EFM vs. Intermittent Auscultation Alfirevic et al 2006 • Increased c-section rate (RR, 1.66; 95% CI, 1.30-2.13) • Increased OVD risk (RR, 1.16; 95% CI, 1.01-1.32) • No change perinatal mortality (RR, 0.85; 95% CI, 0.59-1.23) • Reduced neonatal seizures (RR, 0.50; 95% CI, 0.31-0.80) • No change in CP risk (RR, 1.74; 95% CI, 0.97-3.11)
Why Use EFM? • Logistics • Trials excluded high risk pregnancies
2008 NICHD Workshop on EFM Reporting Multiple discipline groups represented: • Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) • American College of Obstetricians and Gynecologists (ACOG) • The Society for Maternal-Fetal Medicine • Royal College of Obstetricians and Gynaecologists (RCOG) • Society of Obstetricians and Gynaecologists of Canada (SOCG)
2008 Workshop Goals The goals of this workshop were: • Review & update the definitions for FHRT patterns • Assess existing classification systems for interpreting specific FHRT patterns & to make recommendations about a system for use in the U.S. • Make recommendations for research priorities for EFM • Reaffirm definitions from the previous work group of 1997
Pertinent Principles Principles defined in the initial publication in 1997, then reaffirmed in 2008 are as follows: • No distinction between long and short-term (beat to beat) variability • External monitoring devices can adequately assess variability • The features of FHR patterns are categorized as either baseline, periodic, or episodic • Sinusoidal term reserved for the ‘true pattern’ • pseudo-sinusoidal is not defined
Pertinent Principles • Definitions are visual interpretations • Gestational age is considered when evaluating patterns • A complete description of the EFM tracing includes: • baseline • variability • accelerations • deceleration • contractions
Changes & New Terminology from 2008 Workshop Classification of FHR Patterns • Abandon the terms: • Reassuring • Non-Reassuring • Three-tiered Classification System • FHRT may move back and forth between categories
Changes & New Terminology from 2008 Workshop Uterine Activity Definitions Quantified as the number of contractions in a 10 min. window, averaged over 30 min • Normal < 5 contractions in a 10 min. period • Tachysystole > 5 contractions in 10 min. period • Should always be qualified as to the presence or absence of associated FHR decelerations
Changes & New Terminology from 2008 Workshop Tachysystole • Perception of pain is not a reliable indicator of potential implication • Abandon the terms • Hyperstimulation • Hypercontractility • A description of duration, intensity, and resting tone can be described
2008 NICHD Terms & Definitions Abandoned Terms: ¥Short term (beat to beat) & Long Term Variability (assessed as one unit) §Hyperstimulation/Hypercontractility (duration, intensity, relaxation time and Tachysystole used) ∆Pseudo-Sinusoidal Abbreviations: FHR-Fetal Heart Rate, bpm-beats per minute, min-minute, sec-seconds _ Emphasis Added ¤ Indeterminate: Institute interventions to improve tracing & refer to the prior 10 min window.
Baseline • Established by • IA: counting FHR at repeated intervals for at least 30 seconds after uterine contraction • EFM: 2 minutes of interpretable FHR data in at least 10 minutes of monitoring • Rounded to increments of 5 • Normal110-160 • Bradycardia: < 110 for 10 minutes • Tachycardia: >160 for 10 minutes
Bradycardia • Must be distinguished from prolonged deceleration (2-10 minutes) • 90-110 bpm usually innocuous • Variability? • Differentiate from maternal heart rate • Sudden and profound bradycardia is a medical emergency • Drop in maternal oxygenation • Acute impairment of uteroplacental exchange • Prolonged occlusion of the cord • Profound vagal stimulation
Tachycardia • Not associated with fetal hypoxia in absence of decelerations • Increases myocardial oxygen demand
Variability Fluctuations in the FHR over time • Absent: amplitude range undetectable • Minimal: 1-5 bpm • Moderate: 6-25 bpm • Marked: >25 bpm
Moderate Variability • Intact nervous pathway • Predicts adequate fetal oxygenation
Minimal Variability • Fetal sleep cycle • Medication • Fetal acidemia • Previous fetal insult • Fetal neurologic or cardiac congenital anomaly
Absent Variability • Fetal acidemia • Preexisting neurologic insult
Marked Variability • Unknown significance
Accelerations • 15 bpm x 15 seconds • 10 bpm x 10 seconds for < 32 weeks • Predictive of: • adequate fetal oxygenation • pH > 7.19 • Rules out acidemia • 2-10 minutes are “prolonged”
Decelerations • Four types: • Early • Late • Variable • Prolonged • Recurrentif occur with >50% of ctx in 20 min • Intermittentif occur with < 50%
Early Deceleration Visually apparent usually symmetrical gradual decrease and return of the FHR associated with a uterine ctx • Gradual decrease (> 30 sec to nadir) • Nadir occurs with peak of ctx • Head compression • No intervention necessary
Late Deceleration Visually apparent usually symmetrical gradual decrease and return of the FHR associated with a uterine ctx • Gradual decrease (> 30 sec to nadir) • Nadir is after the peak of the ctx • Uteroplacental insufficiency • Initiate intrauterine rescuscitative measures • Variability?
Causes of Uteroplacental Insufficiency Adapted from “Fetal Heart Monitoring: Principles and Practices” AWHONN, 2009
Variable Deceleration Visually abrupt decrease in FHR • < 30 seconds to nadir • Decrease is 15 bpm or greater • Lasts 15 seconds to 2 minutes • Variable in their temporal relationship to ctx • Cord compression • Variability?
Prolonged Deceleration Visually apparent decrease in the FHR below the baseline • Decrease is 15 bpm or greater • Lasts 2-10 minutes Adapted from “Fetal Heart Monitoring: Principles and Practices” AWHONN, 2009