Download
1 / 58
580 likes | 759 Views
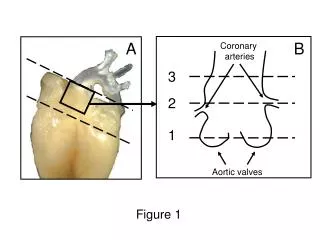
Results of ED Coronary CTA Trials. Udo Hoffmann, MD MPH. Disclosures. Research Grants : Bracco Diagnostics Bayer Healthcare GE Healthcare. Anderson JL et al. Circulation. 2007;116:e148-304. CT is especially suited for the ED setting.

E N D
Results of ED Coronary CTA Trials Udo Hoffmann, MD MPH
Disclosures Research Grants: Bracco Diagnostics Bayer Healthcare GE Healthcare
CT is especially suited for the ED setting • ECG, initial biomarkers, and clinical presentation and traditional risk factors – no safe triage possible (Nagurney, JAMA 2006) • goal in the ED: quick turnover and identification who do NOT need to be admitted • only 20% of patients with ACP have ACS, 80% could be discharged • - requires a fast, available and robust diagnostic imaging test with nearly perfect NPV • CAD – No. 1 cause for ACS (80%-90%) – optimally direct visualization
Coronary Calcium in ACP Patients with uncertain MI and no history of CAD Reference Mod N Sens Spec PPV NPV Laudon et al. Ann Em Med 1999 EBCT 105 1.00 N/A N/A 1.00 McLaughlin et al. Am J Cardi 1999 EBCT 134 0.88 0.37 0.08 0.98 Georgiou et al. JACC 2001 1999 EBCT 192 1.00 0.47 0.26 1.00 ??% of patients have only non-calcified plaque
Important ED coronary CTA studies Hollander et al. 568 patients, none of the discharged subjects (n=476, 84%) who all had absence of significant stenosis (>50%) suffered a cardiovascular event (cardiovascular death, non-fatal myocardial infarction) during a 30-day follow-up period
ROMICAT I – Demographics and Risk Factors Hoffmann et al. JACC 2009
Prevalence of Plaque and Stenosis in ACP CAD categories by CT with relevance for early triage of patients with ACP in the ED (n=368, 8% ACS) Non-obstructive Plaque 31.2% No CAD 50.4% Significant stenosis detected/ not excluded 18.4% Hoffmann et al. JACC 2009
ROMICAT I – CAD and ACS No CAD No ACS Hoffmann et al. JACC 2009
ROMICAT I – CAD and ACS No CAD No ACS Nonobstructive Plaque • 7 ACS • non-stenotic ACS • small vessel disease Hoffmann et al. JACC 2009
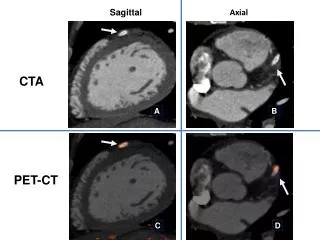
Challenges – small coronary branches 59-year old female with typical chest pain, non-diagnostic ECG and negative serial Troponin
ROMICAT I – CAD and ACS No CAD No ACS Nonobstructive Plaque • 7 ACS • non-stenotic ACS • small vessel disease Significant stenosis detected or not excluded 24 ACS Hoffmann et al. JACC 2009
No ACS No ACS ACS ACS Plaque Sign. Stenosis 31 24 154 44 No Stenosis No Plaque 7 0 183 293 ROMICAT I – Diagnostic Accuracy 1. Triage Criterion: Presence of Plaque Sens: 100% (0.88-1.00) NPV: 100% (0.98-1.00) Spec: 54% (0.49-0.60) PPV: 17% (0.12-0.23) 2. Triage Criterion: Presence of Stenosis (>50%) Sens: 77% (0.59-0.90) NPV: 98% (0.95-0.99) Spec: 87% (0.82-0.90) PPV: 35% (0.24-0.48) Hoffmann et al. JACC 2009
Efficacy of CT - Age and Gender Bamberg et al. AJC 2009
What to do with stenotic lesions? severe RCA lesion
Culprit Lesions Features Non-calcified plaque Positive remodeling Spotty calcification Hoffmann JACC 2006, Motoyama JACC 2007, Kitagawa AHJ 2008
A CT-based Score to Identify Culprit Coronary Lesions Among Patients With Acute Chest Pain and Low to Intermediate Likelihood of ACS Maros Ferencik, Christopher L. Schlett, Khuram A. Nasir, Brian B. Ghoshhajra, Mathias F. Kriegel, Subodh B. Joshi, Ian S. Rogers, Quynh A. Truong, Dahlia Banerji, Fabian Bamberg, Thomas J. Brady, John T. Nagurney, Udo Hoffmann Cardiology Division, Dept. of Radiology and Dept. of Emergency Medicine Cardiac MR PET CT Program Massachusetts General Hospital and Harvard Medical School
Background • Retrospective studies suggest that lesion culprit lesions in ACS patients can be identified by CT and are characterized by • Positive remodeling index • Spotty calcifications • Larger plaque areas • Low CT attenuation of the plaque • However, whether these criteria enable appropriate risk stratification among patients who have significant stenosis is unknown Motoyama S et al. JACC. 2009;54:49 Motoyama S et al. JACC. 2007;50:319 Hoffmann U et al. JACC. 2006;47:1655
Methods – Subject Selection • CT performed in 368 subjects with acute chest pain but without objective evidence of ACS • In 34/368 subjects (9%) at least one >50% stenosis was detected by CT • 21 subjects with ACS • 13 subjects without ACS • culprit vessels/lesions were determined based on combination of available clinical data (nuclear stress test, invasive coronary angiography)
Methods – Characterization of stenotic lesions by Coronary CTA • CT images were analyzed on a dedicated workstation (Vitrea, Vital Images) • Two independent readers analyzed the data, blinded to the clinical information • Measurements • Degree of stenosis • Stenosis length • Remodeling index • Plaque area at the site of the stenosis • Plaque volume • Plaque composition: non-calcified, spotty calcifications, heavy calcification
Results – ROC Analysis Score D Cutoff = 2 Sens 90% Spec 85% PPV 90% NPV 85%
Limitations • Small sample size • Invasive coronary angiography not available for all subjects • IVUS not available for the verification of plaque characteristics • Findings need further validation in a larger sample
Conclusions • Confirmed earlier studies that culprit lesions in ACS are characterized by • positive remodeling, spotty calcifications, larger plaque areas, and low CT attenuation of the plaque • Identified length of stenosis as additional characteristics • Demonstrate high accuracy of a CT-based score for ACS within the subgroup of patients with significant stenosis on coronary CTA • May serve as a triage criterion to decide whether patients with significant stenosis but absence of objective signs of ischemia should be referred to invasive coronary angiography
What to do with stenotic lesions? severe RCA lesion
Stenosis w/o ACS 14/34 patients with a significant stenosis in CT had no ACS or MACE after 6 months
Incremental Value of LV function severe RCA lesion no regional LV dysfunction normal stress SPECT study Discharge diagnosis of ‘non cardiac chest pain’ No MACE after 6 months
Incremental value of LV Function Seneviratne et al. submitted
cardiac CT vs. nuclear stress perfusion imaging in patients at very low risk for ACS (serial negative Troponin measurements) • Outcomes: ACS during index hospitalization and 6 month FU
Outcomes Gold Standard UAP More Interventions in very low risk population
Time to Diagnosis and LOS Shorten LOS and minimize cost
Cardiac CT- Changing Management • presumptive diagnosis and management after standard ED triage with cardiology consultation (n=58) • CCTA was performed and results presented to caregivers who adjusted their recommendations • revised ACS diagnosis in 18 of 41 patients • canceled hospitalizations in 21 of 47 • altered early invasive treatment in 25 of 58 • no MACE events were recorded in the 32 patients discharged from the ED Rubinshtein Circulation 2007
CT will be highly effective because.. • Fast, robust, and available – unique direct visualization of CAD • Strength of CT – high NPV - high Prevalence of negative CT exams (50%) in patients in whom traditional risk assessment does not allow triage • Combined assessment of CAD and regional LVF - Incremental Value of LV function to guide management if CT is positive (modest PPV of CAD findings) • Prognostic benefits – warranty period, preventive therapy
Questions • Absence of CAD justifies discharge without serial Troponin? • Incremental benefit of LV function justifies additional radiation exposure? • CT appropriate for very low, low or intermediate risk ED patients? • CT saves invasive angiograms – i.e. in patients with minimal troponin increase (exclusion of significant CAD in myocarditis) • Change of CT indication by introduction of hs troponin • TRO
Additional Promises of CT - Prognostic Benefits • negative CT – “clean bill” for several years - decrease of subsequent testing in repeated presenters • CT - new non-obstructive disease – initiation of secondary prevention
Incidental findings by CT Lehman et al. American Journal of Medicine 2009
ROMICAT I – Incidental Findings by CT Definite alternative diagnosis: 1.3% pneumonia (n=3), pneumothorax (n=1), and gallstones in a patient with cholecystitis (n 1). Possible alternative diagnosis: 4.1% No PE, AD hiatus hernia (n=12), thoracic aortic aneurysm (n=3), sinus of Valsalva aneurysm (n=1) Subsequent diagnostic testing in 20.5% of patients, with 65/81 for noncalcified nodules Within 6 months, 3 patients underwent biopsies with 2 of the lesions diagnosed as cancer. Lehman et al. American Journal of Medicine 2009
Randomized Trials • CT STAT (16 centers, 700 patients, PI Gil Raff) • CT vs. MPI in low risk patients • sponsor: Bayer Healthcare • ACRIN (4 centers, 1300 patients, PI Harold Litt) • CT vs. SOC in low risk patients • sponsor: ACRIN • ROMICAT II (7 centers, 1000 patients, PI Udo Hoffmann) • CT vs. SOC in intermediate risk patients • sponsor: NHLBI • Outcomes: low health effect size, cost driven, potentially MACE over two years in intermediate risk
CT –STATMulti-center Prospective Randomized design 15 sites experienced with CCTA750 “Low-risk” acute CP patients (TIMI Risk score<4, Initial ECG & Enzymes Normal) James Goldstein, M.D., Kavitha Chinnaiyan, M.D., Daniel Berman, M.D., Udo Hoffmann, M.D., Stephan Achenbach, M.D., Leslee Shaw, Ph.D., Aiden Abidov, M.D., Ph.D., Brian O'Neill, M.D., John Lesser, M.D., Issam Mikati, M.D., Uma Valeti, M.D., Michael Shen, M.D., and Gilbert Raff, M.D., for the CT-STAT investigators
CT STAT - OBJECTIVES • Primary outcome: Diagnostic efficiency - Time-to-diagnosis & cost-to-diagnosis • Secondary outcome: Safety - MACE over 6-months
CCTA Arm Stenoses 0-25% D/C Stenoses >70% ICA Stenosis 26-70%, CAC >100 Agatston units, or uninterp scans MPI CLINICAL DECISION ALGORITHM SOC ARM • Nl serial ECGs cardiac biomarkers and MPI D/C • Abnormal ECG, biomarkers and/or MPI ICA
CLINICAL OUTCOMES: CCTA • No stenosis 297/361 (82.3%) pts • significant stenosis in 27 (7.5%) pts • Moderate stenosis in 23 (7%) pts • CTA uninterpretable in 14 (3.9%) pts • MPI in 37 patients • ICA in 24, revasc in 13 (9 PCI, 4 CABG) • No ACS in patients in whom CCTA excluded stenoses
CLINICAL OUTCOMES: SOC • CCTA in 8 patients • ICA in 21 patients (8 PCI, no CABG)
CLINICAL OUTCOMES: CCTA vs SOC • ICA during index visit (CCTA = 5.1%, SOC = 4.6%, p = NS). • ACS (CCTA = 3.2%, SOC = 3%, p = NS).
TIME-TO-DIAGNOSIS CCTA Reduced Time by 54%, p=0.0001
COSTS-TO-DIAGNOSIS CCTA Reduced Costs by 38%, p=0.0001
CONCLUSIONS • Low risk population – 3% ACS, 86% without significant CAD • Time-to-diagnosis decreased by half, due to more rapid facilitation in testing • Cost-to-diagnosis decreased by one-third, primarily due to expedited time-to-diagnosis and reduced length of stay
Overview of ROMICAT II Randomized controlled diagnostic multi center (n=7) trial, including 1000 subjects with acute chest pain and low to intermediate likelihood of ACS Primary Aim: To demonstrate that including cardiac CT into the early assessment of patients with ACP improves the efficiency of patient management. 50