Download
1 / 12
440 likes | 1.3k Views
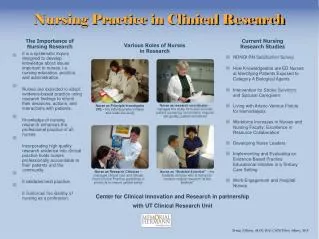
Spirituality in Nursing Practice. Kelly Barker Rachel Gallaher Chassie Turnbow Middle Tennessee State University. What is “Spirituality?”. Religion : The “institutionalization” of like values, beliefs, and lifestyles amongst a shared group of people Spirituality :

E N D
Spirituality in Nursing Practice Kelly Barker Rachel Gallaher Chassie Turnbow Middle Tennessee State University
What is “Spirituality?” Religion: The “institutionalization” of like values, beliefs, and lifestyles amongst a shared group of people Spirituality: “a belief in and experience of a being or state…that transcends physical reality and provides direction, meaning and/or affirmation in one’s life” Spirituality is often forgotten or considered unimportant when it comes to patient care.
What do Patients want? • Research shows that 2/3 of patients would welcome questions regarding their spirituality during their health history. • Research has also shown that when a patient’s spiritual needs are met they experience a greater quality of life.
Spirituality: An Intervention Our specific idea of a nursing intervention was to include spiritual assessment at the beginning of care, a continual assessment of spirituality throughout a plan of care, and participating with a patient in their spiritual care as personally needed. Examples of this would be participating in prayer with a patient.
The Degree to Which Spiritual Needs of Patients Near the End of Life are Met Carla Hermann (2007) This study was a descriptive study of 100 patients over six months in one inpatient and five outpatient hospices in the southeastern United States. Independent needs, such as prayer, were met at a high rate while needs that were dependent upon others, like attending religious services, were often unmet. 68% of the subjects rated their current life satisfaction lower than previous life satisfaction. Hermann firmly encourages the idea of participating with patients to meet their spiritual needs. According to Hermann, “Nurses must assess for spiritual needs with an open mind and be able to assist patients in exploring their needs from a broad perspective.”
Effect of Spirituality on Successful Recovery from Spinal Surgery Hodges, Humphreys, and Eck (2002) • 188 spinal surgery patients were asked to complete a visual analog pain scale (VAS) and the Oswestry functional capacity questionnaire (OSW) pre- and postoperatively. • The results of the study found significant improvements in both VAS and OSW after surgery, but found no correlation between VAS, OSW and INSPIRIT; there was no significance in outcome data related to patient’s spirituality. Even though outcomes were not related to patient’s spirituality, the researchers insist that “strong spirituality can provide the patient…with the determination…to recover from many illnesses. These beliefs should be supported and encouraged by physicians.”
Israeli Oncology Nurses’ Religiosity, Spiritual Well-Being, and Attitudes Toward Spiritual Care: A Path Analysis Musgrave and McFarlane (2004) • This study examines demographic factors and the interceding variables of intrinsic and extrinsic religiosity, as well as “spiritual well-being in Israeli oncology nurses’ attitudes towards patient care.” 167 nurses revealed that their attitudes towards spiritual care were directly influenced by their own spiritual well-being. Musgrave et al. also fervently concluded that “Only one of the antecedent factors – education – had a direct relationship with attitudes toward spiritual care.”
Recommendation & Support of Intervention Regardless of the patient outcome, spirituality “should be supported and encouraged…since they can only be beneficial to a patient’s recovery.” - Hermann • Hodges et al. revealed that the majority of patients want to discuss their spiritual needs during the medical history; this same study also highlighted previous studies that proved increased levels of spirituality have numerous health benefits, such as lower blood pressure and less depression. • Hermann indicated several spiritual activities that patients nearing the end of life would like incorporated into their care: prayer, attending religious services, reading religious texts, and talking with someone about spiritual issues. • Musgrave et al. disclosed that, “Training was associated positively with attitudes toward spiritual care in oncology and hospice nurses.”
Recommendation & Support of Intervention cont. • The cost of incorporating spiritual education into a nursing program (or after graduation) is minimal and the benefits of such a program would far outweigh the costs. Also, nurses should constantly maintain cultural sensitivity regarding spiritual issues and support all patients regardless of their spiritual beliefs. Spiritual acceptance and discussion can be discussed at any time with anyone and only requires a few moments of time. Education is the most critical aspect in the ability to provide quality spiritual care.
Implementing Change • The primary way we would go about introducing our change is making spiritual education part of orientation to a new facility • Another way of incorporating our plan is to include a “Spirituality” assessment box on the initial assessment to be included in their permanent record; this would give patients a chance to voice how important spirituality is to their care and if there are any deficiencies that need to be met. • Some employees will resist this change; however, healthcare professionals need to keep in mind the holistic approach to patient care. No attempt at proselytization would be made. The primary concern is the patient and, as evidenced earlier, attempts to include spirituality in care are only beneficial.
To Conclude… Patient care is of the utmost importance. Anything that can be done to improve their quality of care should be done. Spiritual assessment, cultural and spiritual acceptance, education, and participation are ways that nurses can vastly improve a patient’s quality of care.
References • Armbruster, C.A., Chibnall, J.T., & Legett, S. (2003). Pediatrician Beliefs About Spirituality and Religion in Medicine: Assocations with Clinical Practice. Official Journal of the American Academy of Pediatrics, 111 (3), 227-235. Retrieved March 26, 2007, from the EBSCOHost database. • Hermann, C.P. (2007). The Degree to Which Spiritual Needs of Patients Near the End of Life are Met. Oncology Nursing Forum, 34 (1), 70-78. Retrieved March 2, 2007, from the EBSCOHost database. • Hodges, S.D., Humphreys C., & Eck J.C. Effect of Spirituality on Successful Recovery from Spinal Surgery. Southern Medical Journal, 95.12 (Dec 2002): 1381(4). InfoTrac OneFile. Thomson Gale. Middle Tennessee State University. Retrieved February 12, 2007. • Musgrave, C.F., & McFarlane, E.A. (2004). Israeli Oncology Nurses; Religiosity, Spiritual Well-Being, and Attitudes Toward Spiritual Care: A Path Analysis. Oncology Nursing Forum, 31 (2), 321-327. Retrieved March 2, 2007, from the EBSCOHost database.