Download
1 / 42
440 likes | 675 Views
Cerebral palsy (CP). CP. W & W 1966-1975 Non-specific term that include disorders characterized by early onset and impaired movement and posture. Non-progressive and may include perceptual problems, language deficits, and intellectual involvement. CP. Incidence.

E N D
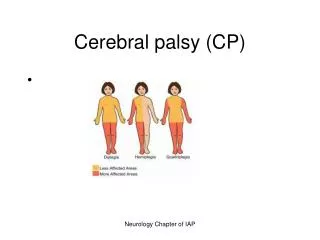
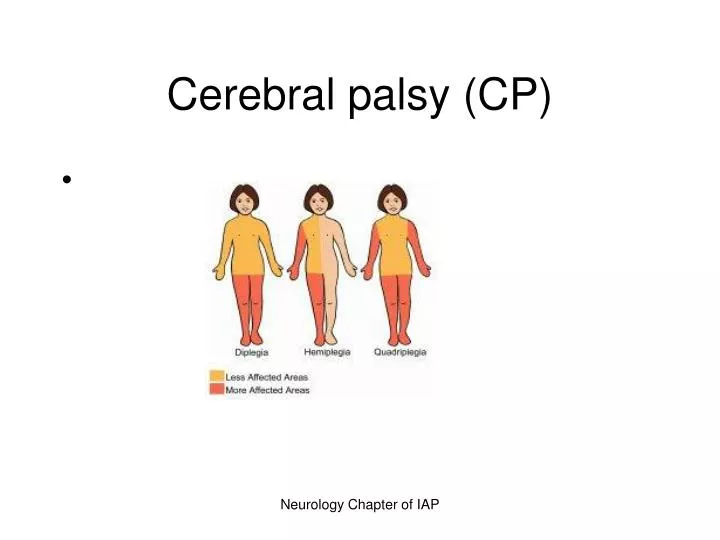
Cerebral palsy (CP) Neurology Chapter of IAP
CP • W & W 1966-1975 • Non-specific term that include disorders characterized by early onset and impaired movement and posture. • Non-progressive and may include perceptual problems, language deficits, and intellectual involvement. Neurology Chapter of IAP
CP Neurology Chapter of IAP
Incidence • Most common physical disability of childhood. • Incidence has increased since the 60’s, maybe due to improved survival of VLBW infants. Neurology Chapter of IAP
Etiology • Variety of perinatal, prenatal, and postnatal factors contribute, either singly or multifactorily to CP. • Commonly thought to be due to birth asphyxia; now known to be due to existing prenatal brain abnormalities. • Premature delivery is the single most important determinant of CP. • In 24% of cases, no cause is found. Neurology Chapter of IAP
Time (% of cases) Prenatal (44%) First trimester Second trimester Causes Teratogens, chromosomal abnormalities, genetic syndromes, brain malformations Intrauterine infections, problems in fetal/placental functioning TABLE 40-1 Causes of CP Neurology Chapter of IAP
Time (% of cases) Labor and delivery (19%) Perinatal (8%) Childhood (5%) Not obvious (24%) Causes Preeclampsia, complications of labor and delivery Sepsis/CNS infection, asphyxia, prematurity Meningitis, traumatic brain injury, toxins Causes of CP Neurology Chapter of IAP
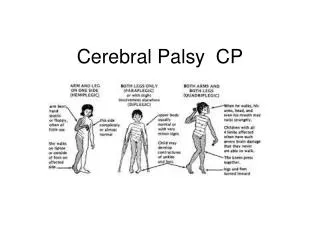
Clinical Classification of CP • Table 40-2, Page 1967. • Spastic-hypertonicity with poor posture control • Dyskinetic/athetoid- abnormal involuntary movement/slow wormlike writhing • Ataxic- wide-based gait • Mixed-type/dystonic- combination of spasticity and athetosis Neurology Chapter of IAP
Clinical manifestations • Delayed gross motor development • A universal manifestation of CP • The discrepancy between motor ability and expected achievement tends to increase as growth advances. • Delayed development of ability to balance slows milestones • Delay in all motor accomplishments Neurology Chapter of IAP
Clinical Manifestations • Abnormal motor performance • Preferential unilateral hand use may be apparent at 6 months. • Hemiplegia, abnormal crawling or asymmetrical crawl; spasticity may cause child to walk and stand on toes • dyskinetic CP or uncoordinated or involuntary movements (writhing tongue, fingers, and toes; facial grimacing), poor sucking and feeding, persistent tongue thrust; head staggering, tremor on reaching, truncal ataxia. Neurology Chapter of IAP
Alterations in muscle tone • Increased or decreased resistance to passive movement (abnormal muscle tone). • Opisthotonic postures or exaggerated back arching, feel stiff on dressing. • Difficulty diapering due to spastic hip adductor muscles and lower extremities • When pulled to a sitting position, child may extend the entire body and be rigid at hip and knee. This is an early sign of spasticity. Neurology Chapter of IAP
Abnormal postures • Children with spastic CP have abnormal posture at rest or when position is changed • Infantile lying prone may have hip higher than trunk with legs and arms drawn in. • Persistent infantile resting and sleeping position is a sign of spasticity. • Hemiparetic child may rest with affected arm adducted and held against torso, with the elbow pronated and slightly flexed and the hand closed. Neurology Chapter of IAP
Reflex Abnormalities • Persistence of primitive infantile reflexes (one of the earliest signs of CP) • Tonic neck reflex • Hyperactivity or moro, plantar, palmar grasp Hyperreflexia, ankle clonus, stretch reflexes can be elicited from any muscle group. Neurology Chapter of IAP
Associated disabilities and problems • Intellectual impairment • 70% w/in normal limits; wide range • Tests should be carried out over a period of time. • Children with athetosis and ataxia more intelligent. Speech difficulties (not a sign or MR)- child has motor and sensory defects ADHD- (may occur)-poor attention span, marked distractibility, hyperactive behavior Neurology Chapter of IAP
ASSOCIATED DISABILITIES Seizures- generalized tonic-clonic;more in postnatally acquired hemiplegia Drooling- may occur and lead to wet clothing/skin irritation Feeding- alterations in muscle tone lead to difficulties chewing, swallowing, talking, etc. Address nutritional concerns. Coughing, choking may lead to aspiration. Altered respiratory patterns may lead to inadequate gas exchange. Neurology Chapter of IAP
Motor Impairment • Orthopedic complications • Unilateral or bilateral hip dislocations, scoliosis, joint contractures due to unbalanced muscle tone. Decreased Mobility • difficulties with toileting may lead to constipation • Difficult chewing bulky foods may lead to constipation • May need stool softeners or laxatives Neurology Chapter of IAP
Associated Problems • Dental carries • Improper dental hygiene • congenital enamel defects (hyperplasia of primary teeth) • high carbohydrate intake and retention • Dietary balance with poor nutritional intake • Inadequate fluoride • Difficulty in mouth closure and drooling • Spastic or clonic movements cause gagging or biting on toothbrush Neurology Chapter of IAP
Associated Problems • Malocclusion in 90% of children • Oral hypersensitivity causes resistance to good hygiene • Gingivitis is secondary to poor hygiene • Dental health further complicated by anti-seizure meds Neurology Chapter of IAP
Associated problems • Nystagmus and amblyopia common • May need surgery or corrective lenses • May be due to sensoneural involvement • Infants lying flat too long may have otitis media which may leads to conductive hearing loss Neurology Chapter of IAP
Diagnostic Studies • Physical Assessment • Observe LBW, preterm, and those with low Apgar scores at 5 minutes. • Observe infants who have seizures, intracranial hemorrhage, metabolic disturbances Neurology Chapter of IAP
DX studies • Since control of movement does not occur until late infancy, dx may not be confirmed until after 6 months of age. • See Box 4-4, page 1968 for warning signs Neurology Chapter of IAP
WARNING SIGNS • Physical Signs • poor head control after 3 months • stiff or rigid arms/legs, arching back, floppy or limp posture • Cannot sit up without support by 8 months • Uses only one side of the body or only the arms to crawl Neurology Chapter of IAP
Warning Signs • Behavioral Signs • Extreme irritability or crying • Failure to smile by 3 months • Feeding difficulties • Persistent gagging or choking when fed • After 6 months of age, tongue pushes soft food out of the mouth. Neurology Chapter of IAP
Therapeutic management • Box 40-5, Wong 1970. • PHYSICAL THERAPY • Most commonly used treatments. • Goal is good skeletal alignment for the spastic child. • For the child with athetosis, training in purposeful acts, even in the face of involuntary motion • Maximum development of proprioceptive sense for the child with ataxia. • Orthotic devices (braces, splints, casting). Neurology Chapter of IAP
OCCUPATIONAL THERAPY • Training in ADL’s along developmental lines. • Sitting to walking; feeding to cooking. • Important to incorporate play into program • Adaptive equipment (utensils for functional use, i.e., eating, writing), computers, etc. Neurology Chapter of IAP
Speech/Language therapy • Early speech training by speech/language pathologist ! • Before child develops poor habits • Advice parents to follow directions of therapist • May need to force child to use tongue/lips in eating Neurology Chapter of IAP
Special Education • Determined by child’s needs • Early intervention programs • Individualized Education Program (IEP) • Specialized learning programs and support services in schools • Socialization to promote self-concept development Neurology Chapter of IAP
Surgical Intervention • Reserved for child who does not respond to conservative therapy! • Or whose spasticity causes progressive deformities Orthopedic surgery • correct contractures or spastic deformities • provide stability for uncontrolled joint • provide balanced muscle power Neurology Chapter of IAP
Surgical Therapy • Tendon-lengthening procedures (heel-cord) • Release of spastic wrist flexor muscles • Correction of hip-adductor muscle spasticity or contracture to improve locomotion • Surgery is for improved function rather than cosmetic reasons and is followed by PT. Neurology Chapter of IAP
Medication Therapy • Little usefulness • Anti-anxiety agents may relieve excessive motion and tension (child with athetosis) • Skeletal muscle relaxants ( methocarbamol (Tobaxin), dantrolene (Dantrium), Baclofen, may be used short-term for older children and adolescents. • Diazepam (Valium) for older children and adolescents, may relieve stiffness and ease motion Neurology Chapter of IAP
Medications • Local nerve blocks to motor points of a muscle with a neurolytic agent (phenol solution) may relieve spasticity. • Botulism toxin (Botox) used to paralyze certain muscles. • Pain • Secondary conditions (seizures, bowel and bladder problems, lung complications). Neurology Chapter of IAP
Service Coordination • Case Management! • Important for collaboration of all health professionals, services, therapies! • Child needs support! • Family needs support! Neurology Chapter of IAP