Download
1 / 85
860 likes | 1.15k Views
Chapter 22. The Pancreas and Diabetes Mellitus. Learning Objectives. Describe pathogenesis and treatment of acute and chronic pancreatitis Describe pathogenesis, manifestations, complications, prognosis of cystic fibrosis Differentiate type 1 and type 2 diabetes mellitus Pathogenesis

E N D
Chapter 22 The Pancreas and Diabetes Mellitus
Learning Objectives • Describe pathogenesis and treatment of acute and chronic pancreatitis • Describe pathogenesis, manifestations, complications, prognosis of cystic fibrosis • Differentiate type 1 and type 2 diabetes mellitus • Pathogenesis • Incidence • Manifestations • Complications • Treatment
Pancreas (1 of 2) • Two glands in one • Digestive gland • Endocrine gland • Exocrine function: exocrine tissue of the pancreas • Concerned solely with digestion • Secretes alkaline pancreatic juice rich in digestive enzymes into the duodenum through the pancreatic duct to aid digestion
Pancreatic Islets • Pancreatic tissue that functions as an endocrine gland • Produce hormones • Beta cells: insulin production • Alpha cells: glucagon • Delta cells: somatostatin
Pancreas (2 of 2) • Endocrine function: endocrine tissue of the pancreas • Consists of multiple small clusters of cells scattered throughout the gland as pancreatic islets or Islets of Langerhans • Discharge secretions directly into the bloodstream • Each islet is composed of different types of cells • Alpha cells: secrete glucagon; raise blood glucose • Beta cells: secrete insulin; lower blood glucose • Delta cells: secrete somatostatin; inhibit secretion of glucagon and insulin
Photomicrograph of pancreatic islet surrounded by exocrine pancreatic tissue.
Acute Pancreatitis (1 of 3) • Pathogenesis • Escape of pancreatic juice from the ducts into the pancreatic tissue • Pancreatic digestive enzymes cause destruction and severe hemorrhage • Involves active secretion of pancreatic juice despite an obstructed pancreatic duct at its entrance into the duodenum • Resulting build-up of pancreatic juice increases pressure within the duct system, causing ducts to rupture
Acute Pancreatitis (2 of 3) • Predisposing factors • Gallbladder disease/gallbladder stones • Common bile duct and common pancreatic duct enter the duodenum via the ampulla of Vater • Impacted stone in ampulla obstructs pancreatic duct • Excessive alcohol consumption • Potent stimulus for pancreatic secretions • Induces edema, spasm of pancreatic sphincter, in ampulla of Vater • Result in high intraductal pressure, duct necrosis, and escape of pancreatic juice
Acute Pancreatitis (3 of 3) • Clinical manifestations • Severe abdominal pain • Seriously ill • High mortality rate
Chronic Pancreatitis • Repeated episodes of mild inflammation of pancreas • Each bout destroys some pancreatic tissue • Inflammation subsides and damaged pancreatic tissue is replaced by scar tissue, leading to progressive destruction of pancreatic tissue • Manifestations • Difficulty digesting and absorbing nutrients • Not enough surviving pancreatic tissue to produce adequate enzymes • Destruction of pancreatic islets may lead to diabetes
Cystic Fibrosis • Autosomal Recessive Disorder • Problem with the gene that codes for a protein known as the Cystic Fibrosis Transmembrane Conductance Regulator • Gene Found on Chromosome 7 at the p31.2 locus • Gene is 230,00 base pairs creating a protein 1,480 AA long • Most common problem is a deletion of three nucleotides – thus causing phenylalanine to not be placed at the 508th position
The protein created by this gene is anchored to the outer membrane of cells in the sweat glands, lungs, pancreas, and other affected organs. The protein spans this membrane and acts as a channel connecting the inner part of the cell (cytoplasm) to the surrounding fluid. • This channel is primarily responsible for controlling the movement of halogens from inside to outside of the cell; however, in the sweat ducts it facilitates the movement of chloride from the sweat into the cytoplasm.
When the CFTR protein does not work, chloride and thiocyanate ([SCN]−). are trapped inside the cells in the airway and outside in the skin. Then hypothiocyanite, OSCN, cannot be produced by immune defense system.
Normally, as primary sweat moves along the duct most of the NaCl is reabsorbed. Reabsorption is driven by a large inward gradient for Na+, which flows into the cell through epithelial Na+ channels (ENaC) in the apical membrane. The basolateral sodium pump then transports Na+ out of the cell and into the blood. Cl- is electrically attracted to Na+ and follows it by flowing through CFTR Cl- channels in the apical membranes of the duct cells; the exit pathway may also be via CFTR.
The duct epithelium has an unusually high conductance for ions and is thought to have a low permeability to water, allowing reabsorption of salt in excess of water. This results in the production of dilute sweat, so that we can be cooled by evaporation without losing an undue amount of salt.
In CF sweat ducts, the Cl- conductance is virtually abolished because CFTR is the only apical pathway for chloride: no other anion channels appear to be in the duct. The sodium conductance also seems to be low, leading to the hypothesis that CFTR activates ENaC in the sweat duct. When Na+ attempts to flow out of a CF duct through remaining sodium-selective pathways, it is unaccompanied by Cl- and so it creates an excess of negative charge in the duct that attracts Na+ and prevents its further absorption.
The net result is that very little NaCl is reabsorbed, resulting in a high salt content in CF sweat. The salt is so high (>100 mM vs. typical values of 20 or 30 mM in healthy individuals, that the sweat chloride concentration is the most reliable single physiological marker of CF.
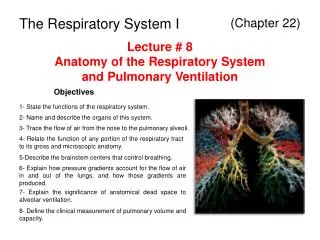
Sweat pore Eccrine gland Sebaceous gland Duct Dermal connective tissue Secretory cells (b) Photomicrograph of a sectioned eccrine gland (220x) Figure 5.5b
Cystic Fibrosis (1 of 3) • Serious hereditary disease, autosomal recessive trait • Mutation of a normal gene, CF gene, on long arm of chromosome 7 • Manifests in infancy and childhood • Incidence in whites: 1 in 3,000 • Incidence in blacks and other races: rare • Mortality, more than 50% die before age 32 • Pathogenesis • Defective transport of chloride, sodium, and H2O across cell membrane • Deficient electrolyte and H2O in the mucus secreted by the pancreas, bile ducts, respiratory tract, and other secretory cells
Cystic Fibrosis (2 of 3) • Pathogenesis • Mucus becomes abnormally thick, precipitates, and forms dense plugs that obstruct the pancreatic ducts, bronchi, bronchioles, and bile ducts • Obstruction of pancreatic ducts: causes atrophy and fibrosis • Obstruction of bronchi: causes lung injury • Obstruction of biliary ducts: causes liver scarring • Abnormal function of sweat glands: unable to conserve sodium and chloride with excessively high salt concentration in sweat; basis of diagnostic test
Cystic Fibrosis (3 of 3) • Treatment • Oral capsules containing pancreatic enzymes to compensate for lack of pancreatic digestive enzymes • Various treatments to preserve as much pulmonary function as possible • Vigorous treatment of pulmonary bacterial infections • Lung transplant may eventually be required if lungs are severely damaged
Low magnification photomicrograph with pancreas of patient with cystic fibrosis.
Diabetes • Inability to regulate blood glucose levels • Type 1 diabetes • Type 2 diabetes • Gestational diabetes • Uncontrolled diabetes can cause nerve damage, kidney damage, blindness, and can be fatal
Diabetes Mellitus • Very common and important metabolic disease • Two major groups depending on cause • Type 1 diabetes • Insulin deficiency • Occurs primarily in children and young adults • Type 2 diabetes • Inadequate response to insulin • Typically an adult-onset diabetes • More common than Type 1 • Becoming more common in children • Manifestation: Increased glucose levels in blood or hyperglycemia
Some Skin Problems Linked to Diabetes • Scleroderma diabeticorum: While rare, this skin problem affects people with type 2 diabetes, causing a thickening of the skin on the back of the neck and upper back. The treatment is to bring your blood sugar level under control. Lotions and moisturizers may help soften skin.
Vitiligo: Vitiligo, a skin problem more commonly associated with type 1 diabetes than type 2 diabetes, affects skin coloration. With vitiligo, the special cells that make pigment (the substance that controls skin color) are destroyed, resulting in patches of discolored skin. Vitiligo often affects the chest and abdomen, but may be found on the face around the mouth, nostrils, and eyes.
Acanthosis nigricans. This is a skin problem that results in the darkening and thickening of certain areas of the skin especially in the skin folds. The skin becomes tan or brown and is sometimes slightly raised and described as velvety. Most often the condition, which typically looks like a small wart, appears on the sides or back of the neck, the armpits, under the breast, and groin. Occasionally the top of the knuckles will have a particularly unusual appearance. Acanthosis nigricans usually strikes people who are very overweight. While there is no cure for acanthosis nigricans, losing weight may improve the skin condition. Acanthosis nigricans usually precedes diabetes and is considered to be a marker for the disease.
Diabetic neuropathies are neuropathic disorders that are associated with diabetes mellitus. These conditions are thought to result from diabetic microvascular injury involving small blood vessels that supply nerves (vasa nervorum) in addition to macrovascular conditions that can culminate in diabetic neuropathy. Relatively common conditions which may be associated with diabetic neuropathy include third nerve palsy; mononeuropathy; mononeuropathy multiplex; diabetic amyotrophy; a painful polyneuropathy; autonomic neuropathy; and thoracoabdominal neuropathy.
Insulin • Influences carbohydrate, protein, and fat metabolism on liver cells, muscle, and adipose tissues • Main stimulus for release: high glucose in blood • Promotes • Entry of glucose into cells • Utilization of glucose as source of energy • Storage of glucose as glycogen • Conversion of glucose into triglycerides • Storage of newly formed triglyceride in fat cells • Entry of amino acids into cells and stimulates protein synthesis
Insulin Actions • Increased glycogen synthesis – insulin forces storage of glucose in liver (and muscle) cells in the form of glycogen; lowered levels of insulin cause liver cells to convert glycogen to glucose and excrete it into the blood. This is the clinical action of insulin, which is directly useful in reducing high blood glucose levels as in diabetes. • Increased fatty acid synthesis – insulin forces fat cells to take in blood lipids, which are converted to triglycerides; lack of insulin causes the reverse.
Increased esterification of fatty acids – forces adipose tissue to make fats (i.e., triglycerides) from fatty acid esters; lack of insulin causes the reverse. • Decreased proteolysis – decreasing the breakdown of protein • Decreased lipolysis – forces reduction in conversion of fat cell lipid stores into blood fatty acids; lack of insulin causes the reverse.
Decreased gluconeogenesis – decreases production of glucose from nonsugar substrates, primarily in the liver (the vast majority of endogenous insulin arriving at the liver never leaves the liver); lack of insulin causes glucose production from assorted substrates in the liver and elsewhere. • Increased amino acid uptake – forces cells to absorb circulating amino acids; lack of insulin inhibits absorption.
Increased potassium uptake – forces cells to absorb serum potassium; lack of insulin inhibits absorption. Insulin's increase in cellular potassium uptake lowers potassium levels in blood.
GLUT1 Is widely distributed in fetal tissues. In the adult, it is expressed at highest levels in erythrocytes and also in the endothelial cells of barrier tissues such as the blood-brain barrier. • GLUT2 Is expressed by renal tubular cells and small intestinal epithelial cells that transport glucose, liver cells and pancreatic β cells. All three monosaccharides are transported from the intestinal mucosal cell into the portal circulation by GLUT2 Is a high-capacity and low-affinity isoform
GLUT3 Expressed mostly in neurons (where it is believed to be the main glucose transporter isoform), and in the placenta. Is a high-affinity isoform • GLUT4 Found in adipose tissues and striated muscle (skeletal muscle and cardiac muscle).
Diabetes—Type 1 • Accounts for 10% of all cases • Body does not produce enough insulin • Causes hyperglycemia (high blood glucose) • Requires insulin injections • May be an autoimmune disease
Type 1 Diabetes Mellitus • Results from damage to pancreatic islets leading to reduction or absence of insulin secretion • Often follows a viral infection that destroys the pancreatic islets • Abnormal immune response may play part: production of autoantibodies directed against islet cells • With a hereditary predisposition • Complication • Diabetic ketosis
Maturity onset diabetes of the young (MODY) refers to any of several hereditary forms of diabetes caused by mutations in an autosomal dominant gene (sex independent, i.e. inherited from any of the parents) disrupting insulin production. MODY is often referred to as "monogenic diabetes" to distinguish it from the more common types of diabetes (especially type 1 and type 2), which involve more complex combinations of causes involving multiple genes (i.e., "polygenic") and environmental factors.
Diabetes—Type 2 • Insulin insensitivity (insulin resistance): cells become less responsive to insulin • Metabolic syndrome: a cluster of risk factors that increase the risk for type 2 diabetes • Once known as adult-onset diabetes • Increasing in children and adolescents