Download
1 / 31
340 likes | 730 Views
Kidney Stones (Urolithiasis, Nephrolithiasis). By: E. Salehifar (PharmD, BCPS). Background. Evidence of stones in a 7000 yo Egyptian mummy Very common (2.7 million visits, >600/000 emergency situations) Men>Women More stones pass out without any intervention

E N D
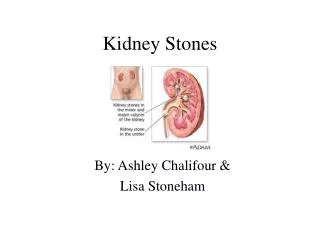
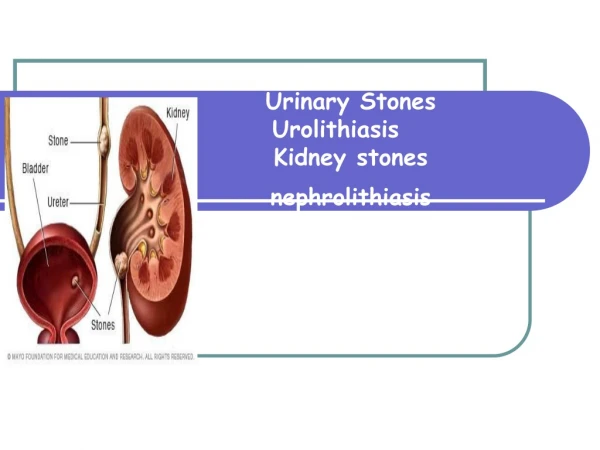
Kidney Stones(Urolithiasis, Nephrolithiasis) By: E. Salehifar (PharmD, BCPS)
Background • Evidence of stones in a 7000 yo Egyptian mummy • Very common (2.7 million visits, >600/000 emergency situations) • Men>Women • More stones pass out without any intervention • Treatment with various techniques
Renal Tract Stones • Calcium • Urate • Cystine • Infection (Struvite) • Others
Calcium Stones • Calcium Oxalate • Calcium Phosphate • Calcium Carbonate
Stone Formation • Causes are unclear • ↑urine concentration of Ca, Oxalate, phosphate, uric acid and cystine • ↓ citrate • Drugs: Loop diuretics, ↑ Vit D, Indinavir • food?, family history, UTI, blockage of the urinary tract, Debris or other crystals • Nephrocalcinosis (mainly in medulla): Hyperparathyroidism, Distal RTA (>70%), cystic kidney disease
Ca Stones Formation • Hypercalciuria (In 50% of nephrolithiasis) • Idiopathic, Hyperparathyroidism, ↑Vit D, Malignancies • associated with obesity & HTN • ↑urine concentration of oxalate • Diet, ileal disease, primary hyperoxaluria type 1 • ↑urine concentration of phosphate • ↓ citrate ( idiopathic, Distal RTA)
Clinical Presentation • Often do not cause any symptoms • Renal colic with intense flank pain often radiating to the groin, burning sensation • Sometimes with nausea, vomiting, hematuria, (fever and chills in infected patients)
Diagnosis • Plain Radiography (Ca, Struvite) • Sonography (size & location of all stone types) • <6 mm pass spontaneously, >1 cm will not • CT Scan • IVP (Intravenous Pyelogram)
Investigations • Exclude bowel disease, diarrhea & the use of antacids and diuretics • Diet assessment: Fluid, protein, Na, Ca, Oxalate, Purine & vit D • Family history • Stone analysis • Baseline: UrineAnalysis,serum Ca, P, urate, BUN, Cr • Recurrent stones: 24-h urine collection • Volume, Osmolality, Ca, P, Oxalate, Citrate, Urate, Na, Cr, pH as well as serum Na, K, Cl, bicarbonate
Prevention • Lifestyle changes • To drink more liquids • Dairy product ?, Calcium pills? • ↓ meat ( patients with acidic urine), ↓ vit D • ↓ Oxalate (beets, chocolate, coffee, cola, nuts, rhubarb, spinach, strawberries, tea, wheat bran)
Treatments • General • Water (>2-3 lit/day), Pain killers • Medical • Surgical • Stone removal • Extracorporeal Shock Wave Lithotripsy (ESWL) • Percutaneous Nephrolithotomy • Ureteroscopic removal
Medical Therapy • Hydrochlrothiazide (with low Na diet) • Allopurinol • Citrate potassium • Thiola and Cuprimine (to ↓ cystine in the urine) • UTI Prevention (after removal of struvites) • Parathyroidectomy
Surgical Treatment • Was necessary until 20 years ago • Recovery time: 4-6 W • Surgery for stone that: • Does not pass after a reasonable time & causes constant pain • Is too large to pass or is caught in a difficult place • Blocks the flow of urine • Causes ongoing UTI • Damages kidney tissue or causes bleeding • Has grown larger (as seen on followup X ray)
Extracorporeal Shock Wave Lithotripsy (ESWL) • The most frequently used procedure • Most need mild anesthesia with short recovery time • Complications: • Hamaturia • Bruising in back or abdomen (ASA should be avoided) • Discomfort caused by stone passage (stent in ureter) • Is not ideal for large stones
Percutaneous Nephrolithotomy(PN or PCN) • For large stone or difficult location for ESWL • Some type of energy probe may be needed to break the large stones • Many need to nephrostomy tube • Hospitalization for several days • Advantage to ESWL: Stone removal by surgeon
Ureteroscopic Stone Removal • For mid and lower ureter stones • Passage of fiberoptic ureteroscope, stone removal by cage-like device or shattering with a shock wave • A small tube or stent may be inserted
Hope Through Research • Why do some people continue to have painful stones? • How can we predict, or screen, those at risk for getting stones? • What are the long-term effects of lithotripsy? • Do genes play a role in stone formation? • What is the natural substance(s) found in the urine that blocks stone formation?
For More Information! • www.afud.org (American Foundation for Urologic Disease) • www.urologyhealth.org (American Urology Association) • www.kidney.org (National Kidney Foundation)