Download
1 / 25
260 likes | 538 Views
THE SOCIAL SCIENCE OF SLEEP DR. SIMON J. WILLIAMS DEPARTMENT OF SOCIOLOGY UNIVERSITY OF WARWICK Email: s.j.williams@warwick.ac.uk. Some quotes to ponder:

E N D
THE SOCIAL SCIENCE OF SLEEP DR. SIMON J. WILLIAMS DEPARTMENT OF SOCIOLOGY UNIVERSITY OF WARWICK Email: s.j.williams@warwick.ac.uk
Some quotes to ponder: • Blessings on him [sic] that invented sleep, the mantle that covers all human thoughts, the food that satisfies hunger, the drink that slakes thirst, the fire that warms cold, the cold that moderates heat, and, lastly, the common currency that buys all things, the balance and weight that equalises the shepherd and the king, the simpleton and the sage (Cervantes, Don Quixote) • Sleep is that golden chain that ties health and our bodies together (Thomas Dekker, The Guls Horne Book (1609)) • Dochtūir na sláinte an codladh (Health’s doctors is sleep)
In this session we shall examine; • Historical and cross-cultural variations in sleeping patterns and practices • Evidence for and against the thesis people in contemporary society are (chronically) sleep deprived • The relationship between ageing, gender and sleep as an illustration of the contribution the social sciences can make to the study of sleep.
Starting points • Sleep is a basic human right, recognised or not • Sleep is crucial to health, well-being and social functioning • Sleep is a form of (learnt) behaviour, involving a complex interplay of biological, psychological, social and cultural factors
Starting points… • How we sleep, when we sleep, where we sleep, what we make of sleep, and who we sleep with, are all socially, culturally and historically variable. • To understand people’s sleep behaviour we need to place it in the context of their everyday/night lives: need to look at the meanings, methods, motives and management of sleep • Limited work to date on the social, cultural and historical dimensions of sleep, however, compared to research in sleep science and sleep medicine
Sleep through the centuries • Sleep has become more privatised, hidden away behind the scenes of social life…the bedroom has become one of the most private and intimate areas of human life • Sleep was a more ‘public’ affair in medieval times: daytime sleep common, in any place that was convenient, sharing of physical sleeping space, sleeping with more than one bedfellow, particularly in lower social ranks. • Sleep in past centuries often a precarious affair: many potential disturbances, including unwelcome intrusions, frigid temperatures, annoying noises, voracious insects (bed bugs), physical maladies, persistent (dental) pain (dulled by alcohol)
Sleep through the centuries… • Improved sleep quality compared to our ancestors, but diminished sleep quantity? • Commonly cited ‘sleep thieves’: Edison’s electric light bulb (extending our days, shortening our nights), changing nature of work (shift work, job intensification etc.), expanding leisure and entertainment opportunities, advent of the 24/7 society, globalisation.
Sleeping cultures/cultures of sleep • Important cultural as well as historical variations in sleep patterns and practices. Three main types of sleeping cultures/cultures of sleep (Steger and Brunt 2003): • Monophasic: consolidation of sleep into one solid block (with a widespread ideal of an 8 hour nocturnal phase), evident in Northern Europe and North America • Bi-phasic or siesta cultures: with a short afternoon nap and a longer night-time sleep, evident in Spain and societies with a Spanish cultural influence • Polyphasic: characteristic of ‘napping cultures’, with ‘anchor’ sleep at night and individual daytime napping as and when the situation allows. Evident in China and Japan.
Sleep cultures/cultures of sleep… • Napping increasingly being encouraged/promoted in the workplace in Northern Europe and North America as the ‘smart’ or ‘efficient’ way to sleep in present day 24 hour economies • Greater uptake in cognitive rather than manual occupations: a new form of inequality in the workplace? • Student presentation of the Siesta/Nap…
Are we (chronically) sleep deprived? • Evidence comes in many shapes and sizes; methodological problems of comparability between studies (different definitions and measures used), ‘normalisation’ of sleepiness within the community? • Levels of (excessive) daytime sleepiness found in various studies: • 32% of American adults scored a significant level of sleepiness on the Epworth Sleepiness Scale in the NSF Sleepiness in America (1997) survey • More than one fifth of UK adults say they have ‘severe’ daytime sleepiness (Leadbeater and Wilsdon 2003)
Are we (chronically) sleep deprived…? • 17% of Finns report daytime sleepiness ‘often’ or ‘always’ (Hyppä and Kronholm 1997) • 21% of Poles feel ‘moderately sleepy during the day’ (Zielinski et al. 1998) • Excessive daytime sleepiness detected in 11% of Australian adults (Johns and Hocking 1997). • More likely in women than men, and in school aged children or young adults than in middle age adults (Partienen and Hublin 2000)
Are we (chronically) sleep deprived…? • Historical evidence that (excessive) daytime sleepiness has risen over the years, and that on average each of us sleeps approx. 1.5 hours less than people at the turn of the twentieth century (Webb and Agnew 1975, Bliwise 1996) • American adults, according to NSF figures, sleep on average only 6.9 hours during the week, rising to 7.5 at weekends (NSF 2002) • Blaxter’s (1990) Health and Lifestyle survey found the population of adults in England, Wales and Scotland almost ‘evenly divided’ between those who claimed to sleep for 7-8 hours per night, those who ‘usually’ slept for less, and those who ‘usually’ had longer hours
Are we (chronically) sleep deprived…? • Overall, it is claimed, current research evidence: • ‘leaves little doubt that most adults, in the USA, UK and other industrialised nations get substantially less than eight hours sleep most nights of the week and many get less than seven’ (Martin 2003: 22) • But does this really matter? Isn’t the recommended 8 hours of shut-eye pretty much a myth anyway?
Are we (chronically) sleep deprived…? • When asked, many people think they aren’t getting enough sleep, due to busy lives/squeezed timetables…A recent UK ‘Precious Time Poll’, for example, found 52% of adults surveyed said they would rather have more sleep than more sex if they had an extra hour in bed! • Laboratory studies indicate that most people (without external interference) sleep between 8 and 9 hours per night (Webb and Agnew 1975, Bonnet and Arnaud 1995) • Evidence suggests that even modest amounts of daily sleep loss accumulate as sleep debt that manifests itself as an increased tendency to fall asleep and reduced levels of psychomotor performance… • Links between sleepiness and accidents, health and public safety…e.g. ‘drowsy driving’ as dangerous as ‘drunk driving’…
Are we (chronically) sleep deprived…? • What role do sleep disorders play? • An estimated 40 million Americans suffering from sleep disorders and a futher 20-30 million suffering from sleep problems, many undiagnosed and untreated (National Commission on Sleep Disorders Research 1992) • Relationship between sleep disorders, sleep disruption and sleep deprivation is complex and contingent • Many other factors, besides sleep disorders, result in sleep disruption and sleep deprivation
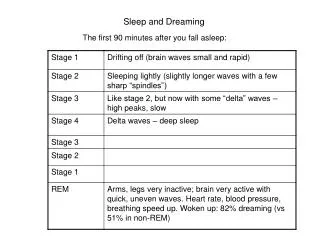
What role do sleep disorders play…? • Many different types of sleep problems and sleep disorders: • dysomnias: disorders initiating/maintaining sleep (e.g. insomnias) and the disorders of excessive sleepiness (e.g. hypersomnias, narcolepsy and obstructive sleep apneoa) • parasomnias: disorders that do not primarily cause a complaint of insomnia or excessive sleepiness (e.g. sleep walking, sleep talking, nightmares, sleep paralysis, bruxism) • Sleep disorders associated with medical or psychiatric disorders (e.g. chronic obstructive pulmonary disease, sleep related gastroesphageal reflux, psychoses, mood disorders)
What role do sleep disorders play…? • Proposed sleep disorders insufficient information to confirm their acceptance as definite sleep disorders(such as short sleeper, long sleeper, menstrual associated and pregnancy associated sleep disorder) • Variations in sleep problems/disorders: e.g. gender (insomnia 1.5 times more common in women than men); occupation, links between work-stress, burnout and insomnia etc. • See Partinen and Hublin (2000) for a review of the epidemiology of these sleep disorders
Are we (chronically) sleep deprived…? • Muddying the water: • Evidence that ‘long’ (i.e 9 hours of more) as well as ‘short’ (i.e. 6 hours of less) have increased mortality risks (Wingard and Berkman 1983, Kripke et al. 1979), even when health status is controlled for… • Most people are not in fact chronically sleep deprived, Harrison and Horne (1995) claim, but have the capacity to take more sleep, in much the same way as eating or drinking in excess of physiological need • Sleeping beyond one’s ‘norm’ produces only marginal benefits for the majority of population • The ability to extend one’s sleep time is not itself hard evidence of the need for this extension
Are we (chronically) sleep deprived…? • The social and environmental contexts of sleep allow for considerable intraindividual variation in sleep duration and structure • Without bringing appreciable improvements in subjective well-being throughout the day, ‘many people are unlikely to be persuaded easily about the benefits of their changing daily sleep/wake pattern in order to take more sleep’ (Harrison and Horne 1995: 901-2)
SO: Are we (chronically) sleep deprived…? • What do you think? • Are you (chronically) sleep deprived • Discussion…Sleep diaries…Epworth sleepiness scores… • Break
Ageing, Gender and Sleep • The relationship between sleep and ageing is a product of both biological and social factors, which in turn need dividing into direct and indirect influences (Morgan 1987) • Biological factors • Direct influences: Age related changes associated with the physiological mechanisms of sleep…Sleep becomes shorter, lighter, more broken, more vulnerable to disruptions and less satisfying as we get older • Indirect influences: Associated with painful, discomforting disease, and other senescent changes…
Ageing, Gender and Sleep… • Social factors: • Indirect influences: changing social roles, relationships, responsibilities, financial factors, bereavement, loneliness/isolation, institutionalisation etc…
Ageing, Gender and Sleep… • What role does gender play across the life course? • Are women disadvantaged in their access to the sleep role as a right and resource in their lives? • Student presentation of Hislop and Arber’s (2003) study of ageing, gender and sleep…
Findings from Hislop and Arber’s (2003) study on gender roles, relationships and sleep: • Methods • Qualitative research on the sleep of women aged 60 and over, including four focus groups (n = 34) and in-depth interviews with a further 28 women, plus audio tape sleep diaries • Findings: • Interactional nature of the sleep relationship for couples, and its effects on sleep disruption in later life • Intrusions into women’s sleep from partners, compounded by women’s own health problems, and by the emotional labour expended in caring for partner’s health and well-being • Sleep influences and is influenced by gendered roles, relationships and life course transitions
Conclusions • Sleep patterns and practices are socially, culturally and historically variable: a complex form of (learnt) behaviour • The (chronic) sleep deprivation debate is far from settled…Arguments and evidence both for and against… • Important changes in sleep as we age; a product of direct and indirect biological factors and indirect social factors. • Women may be disadvantaged in terms of their access to the sleep role, as a right and resource across the lifecourse • END