Download
1 / 16
160 likes | 392 Views
A risk-benefit analysis of celecoxib for the prevention of colorectal cancer. James Cross, MS Pharmaceutical Outcomes Research and Policy Program University of Washington ----- Biobehavioral Cancer Fellows Day April 20, 2007. The framework & decision problem.

E N D
A risk-benefit analysis of celecoxib for the prevention of colorectal cancer James Cross, MS Pharmaceutical Outcomes Research and Policy Program University of Washington ----- Biobehavioral Cancer Fellows Day April 20, 2007
The framework & decision problem • Nonsteroidal antiinflammatories (NSAIDs) risk of colorectal adenoma. • NSAIDs risk of gastrointestinal & cardiovascular adverse events. • What is the risk-benefit profile of these drugs for colorectal cancer chemoprevention?
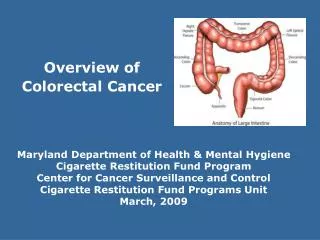
Colorectal cancer: US estimates for 20061 • Lifetime risk: 1 in 18 diagnosed with CRC. • Diagnoses: 148,610 • Deaths: 55,170 • 1 Ries L et al. SEER Cancer Statistics Review, 1975-2003, NCI. Bethesda MD. http://seer.cancer.gov/csr/1975_2003/ Based on November 2005 SEER data submission.
Polyps: precursors to adenocarcinoma Standard colonoscopy Colonoscopy: current surveillance method among “high-risk” patients. Zielinski SL. JNCI 2004.
NSAIDs • Non-selective inhibitors • Ibuprofen, naproxen, diclofenac • Aspirin • COX-2 selective inhibitors • Celecoxib
Inflammation in colorectal cancer Ulrich C, Nat Rev Cancer 2006
Evidence of benefit:NSAID vs. placebo at 3 years 1Baron JA, NEJM 2003 2Bertagnolli MM, NEJM 2006 3Arber N, NEJM 2006.
Evidence of risk (CV, GI) • GI bleed risk for ASA: • OR: 1.59 (1.40-1.81)1 • OR: 1.77 (1.07-2.94)2 • CV risk for Celecoxib: 1Derry L BMJ 2000. (RCT meta-analysis, n=66,000) 2USPhysician Health Study NEJM 1989. 3 Solomon SD Circulation 2006.
Current opinion of celecoxib …Due to the increased risk of CV events associated with their use, COX-2 inhibitors are not recommended routinely for sporadic adenomas. -Practice Guideline in Oncology v1.2007, Nat’l Comprehensive Cancer Network …It is reasonable to conclude that celecoxib has no role as a chemopreventive agent either in patients with nonfamilial colonic adenomas or the general population. -Psaty and Potter NEJM 2006
Reasons for doing a risk benefit analysis • Proposed risks: • Cardiovascular (celecoxib) • Gastrointestinal (aspirin) • Proposed benefits: • Colonoscopies not perfectly sensitive • Slows carcinogenesis process • Decreases # of adenomas • Decision problems: • Efficacy data based on surrogate endpoint • No methodical, quantitative assessment
Risk benefit analysis: methods • Objective: • compare the net health outcomes (risk & benefit) between 3 CRC prevention strategies • ASA vs celecoxib vs colonoscopy alone • Perspective: • societal perspective, 20 years • Population: • 60 years, prior finding of adenoma • Approach: • health-state transition model quantifying health outcomes over 20 year period
Health-state transition model of CRC prevention Polyp free (Post-polypectomy) Advanced adenoma Death CRC GI Tox Discontinue ASA/COX CV Tox
Methods: Model assumptions • GI/CV serious adverse events require drug discontinuation. • Those who discontinue drug assume health state transitions as though they were receiving only colonoscopy.
Results: Net health impact # cancer case/death + # cardiovascular event/death = net health impact COMPARATOR[net health impact – REFERENCE[net health impact] • For a cohort of 100,000 (undiscounted):
Limitations • Scarcity of data: • correlation between surrogate endpoints and outcomes used in decision-making. How should this be handled here, & in general? • ASA use: • How best to model cardioprotective effect of ASA use, which celecoxib users may also take? • For calculations, 1 cancer case/death = 1 GI/CV event.
Acknowledgements • Dissertation committee: • Lou Garrison (UW, chair) • Scott Ramsey (UW & FHCRC) • Dave Veenstra (UW) • Funding: • Biobehavioral Cancer Prevention & Control Training Program (NCI & UW)