Download
1 / 64
680 likes | 1.03k Views
Celiac Disease Yes, It is Here!. Larry E Lyon M.D. Sioux Valley Clinic Luverne October, 2005. Introduction. Celiac disease has been considered to be rare Many new studies and new data show that it is far more common than thought previously

E N D
CeliacDiseaseYes, It is Here! Larry E Lyon M.D. Sioux Valley Clinic Luverne October, 2005
Introduction • Celiac disease has been considered to be rare • Many new studies and new data show that it is far more common than thought previously • Also now aware that it is multisystem disease not just gastrointestinal disorder
Background • Autoimmune reaction to a protein called gluten found in certain grains • Reaction leads to damage of small intestine resulting in malabsorption and a variety of clinical manifestations • Also called celiac sprue, sprue or gluten induced enteropathy • Not an allergy: T-cell mediated, not IgE IgE reaction: angioedema, urticaria, bronchospasm
History • 1888: Samuel Gee described illness that could be regulated by diet • 1950: Dr. Dicke from Netherlands noted that his young patients with diarrhea improved when wheat was in short supply in World War II, got worse when wheat was reintroduced • 1954: Paulley described biopsy changes
History-Continued • 1955:Small bowel biopsy tube • 1960: Skin condition called Dermatitis Herpetiformis also found to have same cause and looked the same on intestinal biopsy • 1970: Genetic link was found and also realized that immune system was involved
Cofactors • Genetic predisposition • Exposure to gluten (prolamins - alcohol soluable) • Wheat (gliadin) • Rye (secalin) • Barley (hordein) • Oats: controversial • Precipitating event, “trigger event” such as infection, pregnency or surgery • New data: Male/Female nearly equal numbers
Prevalence • Much more common than previously thought (1 in 4,000 or 5,000) • Recent antibody studies: 1 in 133 - U.S. • 30,000 now diagnosed in U.S. • 3,000,000 projected prevalence in U.S. • Much more uniform world-wide than realized but still variability • New data led to NIH calling for Consensus Development Conference
National Institutes of Health Consensus Conference • June, 2004 • Conference with national and world experts • Prevalence of 1% of U.S. population • Disease is widely underrecognized
Prevalence-Continued • First degree relative - 5-12% • Second degree relative - 3% • Italy - CD has been considered common; all children are screened by age 6 • Ireland: 1 in 122 • North African refugee population • 1 in 20
Prevalence-Continued • One of the most common genetic based diseases ever described • Diabetes mellitus • 18 million patients in U.S. • 1 in 3 not diagnosed
Pathophysiology • Gluten ingestion interacts with antibody • Reaction actually damages the lining of the small bowel, primarily duodenum • Villi become shortened, then flat • Patchy areas of involvement- may skip • 34% of celiacs show classic flat mucosa • Duodenum is source of absorption of nutrients, iron, calcium, fat-soluable vitamins, folic acid
Celiac Disease Histology Partial atrophy II Partial atrophy I Normal Partial atrophy III Total atrophy Subtotal atrophy
Diagnostic Criteria • European Society of Pediatric Gastroenterology and Nutrition has set international standards - extrapolated to adults • Interlaken 1969 - 5 step process with 3 biopsies • Budapest 1990 - Less restrictive • 1. Positive duodenal biopsy • 2. Clinical remission with gluten free diet
Diagnostic Small Bowel Changes • Increased intra-epithelial lymphocytes • Elongated crypts • Varying degrees of villous atrophy found in celiac disease • In adults these changes found in celiac sprue, tropical sprue, graft vs host reaction, giardiasis and HIV enteropathy • In infants, cow’s milk allergy and gastroenteritis can look similar
Marsh Classification • 0. Normal • 1. Increased intraepithelial lymphocytes • 2. Cryptic hyperplasia • 3. Partial villous atrophy • 4. Total villous atrophy • Prefer to identify 3 well oriented crypt to villous units to interpret villous atrophy
Presentation Forms • 1. Classic • 2. Late Onset • 3. Extraintestinal/Atypical • 4. Asymptomatic/Silent • 5. Associated conditions • 6. Latent
1. Classic-Infants • May appear at 4-24 months of age • Failure to thrive, developmental delay • Diarrhea and or vomiting • Abdominal distention • Irritability, fatigue • Malnutrition, palor, edema, anemia • May develop tolerance in adolescence and reappear in adulthood
2. Late Onset • Teens or adults- age variable • Symptoms (in the past) mainly GI - diarrhea and malabsorption • Bloating, flatulence,dyspepsia, abdominal pain (recurrent or chronic) • Fatigue • Constipation in 10-20%
Late Onset (Continued) • May mimic irritable bowel syndrome - Up to 20% of those diagnosed with IBS may have celiac disease • 35-40% of celiacs have been diagnosed earlier with IBS
3. Extraintestinal-Atypical • Now over 50% of Celiac patients • Unexplained anemia (~10% with upper endoscopy for anemia will have Sprue) • Folic acid, Vitamin B12 deficiencies • Arthralgias • Peripheral neuropathy, seizures, ataxia • Bone pain, osteoporosis • Glossitis, stomatitis
Extraintestinal-Atypical • Dermatitis herpetiformis- 10% of CD • Short stature- 10% will have CD • Netherlands requires small bowel bx • Reproductive • Delayed onset of puberty • Infertility (both male and female) • In Europe CD is in Differential Diagnosis • Recurrent miscarriages or fetal loss
Extraintestinal-Atypical • Fatigue • Elevated transaminases • Dental enamel hypoplasia
4. Silent/Asymptomatic • Antibody tests will be positive • Small bowel biopsy is positive • Still at risk for complications of celiac disease • Usually 1st or 2nd degree relative of pt with CD who has screening test done • Symptomatic patients may be “tip of the iceberg”
5. Associated Conditions • Diabetes mellitus Type 1 (3-8%) • Autoimmune thyroid disease - 5% • Rheumatoid arthritis • Sjogren’s syndrome • Systemic lupus erythematosus (SLE) • Trisomy 21: 5-12% will develop sprue • Primary biliary cirrhosis (6%) • 50% of celiacs have lactose intolerance
Associated Conditions • Turner’s Syndrome - Single Female X • Williams syndrome - Partial deletion of chromosome 7 • Approximately 30% of Celiacs diagnosed after age 20 yr old will have some type of autoimmine disease
6. Latent Celiac Disease • Antibody test positive • Biopsy negative • May need “trigger event”
Clinical Diagnosis • History still paramount importance • Need to think of it • Antibody tests supportive, not essential • Gastroscopy with duodenal biopsy • Response to gluten free diet • Europe - 2-3 weeks to diagnosis • United States- 10 years to diagnosis
Small Bowel Biopsy • Gold standard for diagnosing celiac sprue • Upper endoscopy (gastroscopy) • Duodenal biopsies - mid & distal • Multiple biopsies necessary • At least 4-6 biopsy pieces need to be taken • Abnormal findings may skip areas • CD3 immunostaining for counting IEL is now possible
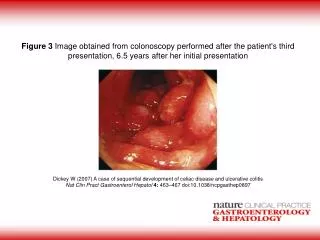
Small Bowel Changes • Colonoscopy, barium enema are normal • Celiac disease primarily involves the small bowel (can involve colon and stomach in severe cases)
Antigliadin Antibody • Older test-1980 • Made by plasma cells, IgA or IgG • AGA-IgG: 57-100% Sensitive 69-87% Specificity • AGA-IgA: 54-100% Sensitive 79-100% Specific • Best tests if less than 5 years old
Antiendomysial Antibody • IgA-Developed in 1990 • 87-95% Sensitive • 95-100% Specific • Immunofluorescence of monkey esophagus or human umbilical cord • Technically difficult • Operator interpretation • Titers correlate with severity of villous atrophy
Tissue Transglutaminase-IgA • Newest antibody test-2000 • IgA • tTG is the autoantigen for the endomysial antibody (but does not require monkey tissue or human umbilical cord) • Now human recombinant source • 84-100% sensitive (some say 75%) • 91-100% specific (some say 75-80%)
Tissue TransglutaminaseIgA-tTG • Titers correlate with severity of villous atrophy • Patients with partial villous atrophy may not have antibodies against tTg or endomysium, but usually gliadin antibody positive • Not always concordance between EMA and tTG antibody- up to 1/3 of patients will have only one of these antibodies
tTG Antibody • May have false positive if another autoimmune disease is present • Chronic liver disease • Inflammatory bowel disease • Diabetes mellitus Type 1
Genetic Studies • HLA (human leukocyte antigen) tissue typing- will be DQ2 or DQ8 haplotype • DQ2 present in 95% of celiacs • DQ8 present in 4-5% of celiacs • Also present in 40% of general population • If not DQ2 or DQ8 will never (or rarely) develop CD
Antibodies • 2-4% of patients with celiac disease have deficiency of IgA (10 times more common than those without sprue) • IgA antibody tests will be negative • Antibody levels will decrease within 2 to 3 weeks of gluten free diet
Possible Laboratory Abnormalities • CBC, platelet count - hyposplenism possible • Vitamin B12 and folate levels • Serum iron, IBC, ferritin levels • Calcium, phosphate, albumin, protein, magnesium • Antiendomysial or antitransglutaminase antibodies (IgA) • Antigliadin antibodies (IgA and IgG) • Blood sugar, thyroid function studies, IgA levels, bone density abnormalities
Dermatitis Herpetiformis • Intensely pruritic rash on elbow, forearm, knee, buttock or scalp • Skin biopsy is diagnostic - granular IgA deposits in dermal papillary tips • Direct immunofluorescence technique • Use formalin free preservative- do not use formalin • Biopsy is done on perilesional skin - not the lesion • Will still have duodenal changes if biopsied
Dermatitis Herpetiformis • Responds to gluten free diet • Rare in children • Occasionally need medication for rash • Dapsone may be needed initially
Diagnostic Steps • If highly suspicious do Small Bowel Bx • If gastroscopy is done do Small Bowel Bx • Less likelyhood - do blood tests • Screening family members • Screening associated conditions • Do Blood tests and biopsies on a gluten containing diet
Blood Test Costs • Antigliadin IgA and IgG Abs - $57 each • Tissue transglutaminase IgA - $204 • Endomysial IgA Ab - $210 • Total IgA level - $39 • Celiac Panel - all above tests - $425 • SVCL Code 2066 (goes to Prometheus Lab) • Preferable to do whole panel if possible
Treatment • Diet, Diet, Diet - Gluten free diet • Consultation with a dietitian • Local support group is valuable • Avoid wheat, rye, barley (and possibly oats) and their products • Oats may be contaminated in field or in preparation • Zero tolerance is best - any gluten (no matter how small an amount) can damage the intestine
Treatment • Gluten-free products available • Some available locally • Internet • Meats, vegetables, fruit and most dairy products (if not lactose intolerant) • Ensure medications are gluten free • Advise bone density test • Vitamin B12 and Folic acid levels • Vitamin, calcium supplements
Response to Treatment • Many will improve within 1-2 days of starting gluten free diet • Antibody levels decrease in 2-3 weeks • May take 3-6 months (sometimes longer) for the small intestine to heal
Hidden Sources of Gluten • Food additives,preservatives, stabilizers • Salad dressings, marinating sauces • Some brands of ketchup, mouthwash • Beer and many other alcohols • Varieties of wheat: spelt, semolina • Medications,glue on stamps and envelopes, vitamins may have a wheat filler or binder