Download
1 / 19
190 likes | 195 Views
Experiences and perceptions of PrEP among gay, MSM, and TGW in the PROUD study in England. Mitzy Gafos , Will Nutland, Sonali Wayal , Gill Bell, Mike Rayment , Caroline Rae, Sheena McCormack and Rob Horne, on behalf of the PROUD study. IAS, 23-26 July 2017, Paris, France.

E N D
Experiences and perceptions of PrEP among gay, MSM, and TGW in the PROUD study in England MitzyGafos, Will Nutland, SonaliWayal, Gill Bell, Mike Rayment, Caroline Rae, Sheena McCormack and Rob Horne, on behalf of the PROUD study IAS, 23-26 July 2017, Paris, France
PROUD (Nov12-Nov16) HIV negative, G/MSM/TGW reporting condomless anal sex last/next 90days; 18+; clinic attendee; willing to take a pill every day Enrolled 544 Risk reduction includes Truvada AFTER 12M Randomised 269 Risk reduction includes Truvada NOW Randomised 275 Follow 3 monthly Endpoint: HIV infection in first 12 months Impact on sexual behaviour and other STIs
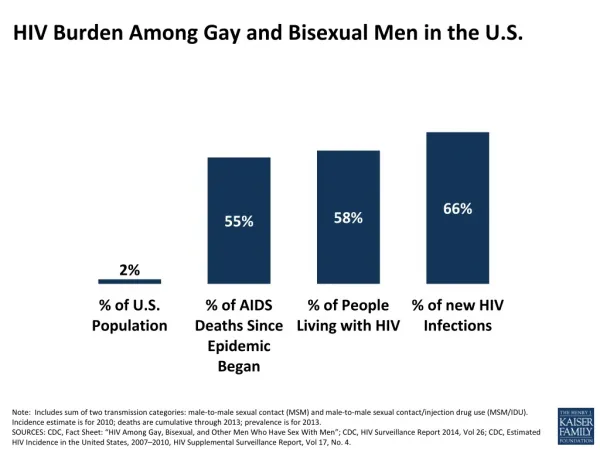
Background • PROUD attracted a high-risk cohort of MSM accessing sexual health services • Eligibility: condomless sex • STI: 33% rectal NG/CT • HIV: 9 per 100pys in no-PrEP group • PROUD demonstrated 86% reduction • We explore PROUD participants' experiences and perceptions of PrEP in relation to other risk reduction strategies.
Methods • 41 semi-structured IDIs (Feb14-Jan15) • Used PrEP: 19/20 in immediate & 14/21 in deferred • Purposive sampling based on self-reported: • Adherence (high/low) • Risk behaviour (increase/same-decrease) • IDIs digitally recorded, transcribed and analysed in NVivo using framework analysis.
‘Rules’ of sex “It slightlyloosens the boundaries rather than taking them off altogether”
“I have a partner who is HIV positive and we have gone without condoms since being on the study which we wouldn’t do before” Impact of PrEP on behaviour “I have definitely experienced more as a bottom since, still very small as a percentage …. but I am more relaxed about allowing a guy to fuck me” “I was selecting negative… I am more looking at the person now... not if they're positive” “I haven’t changed the way I think because I am taking this pill.. having these pills doesn’t give me an excuse to be more crazy than I already am” “I’ve taken the medication and obviously I’ve still had intercourse in the way that I would if I’ve not taken the tablet … my behaviours have remained the same” “There is no marked difference, I was having a huge amount of condomless sex before”
Perceptions of PrEP “It is a security blanket” “What i do for work (sex work) it is a major safety net” “I feel like there is this protective bubble around me” “It is like a defence mechanism, you know, don’t tempt fate” “It is a belt and braces thing” “I wear a crash helmet when I go on my bicycle and seemed sensible under the current circumstances to use the medication”
Psychosocial benefits “The feeling of relief of 25 years of weight, of stress.. where every sexual interaction is a wave of risk” “PrEP has replaced fear as the central focus of relationships” “For the first time in my life since I started taking it I actually have had sex as I like it without having thishorrible feeling of ‘my god’ after” “Worry obviously ruins the sexual experience.. removing ..that worry.. probably improved my life overthe past 2 years
Psychosocial benefits “There is more intimacy not using the condoms and the tablets can prevent me from getting HIV” “The whole experience has really made me quite.. liberated” “It gives you the peace of mind the added control of minimising that risk” “Its been very good for my mental health (ADHD) because I’ve not had to associate sex with danger so much which is good”. “If I wasn’t taking it, sooner or later the inevitable is going to happen”
“I had bare-backed the last 25-30yrs and never had a single STI.. in the last 18mths I have had syphilis and gonorrhoea 3 times… what has changed is I now live and work in London for half the week” Social context of ‘risk’ “On Gaydar or Grindr… you have 13 or 14 people messaging you within 2 hours of arrival, so I did go.. through the ‘child in a sweet shop syndrome’” “I have got more into bareback as a result of getting more into chemsex… for me the pleasure of bareback sex outweighs the risk of contracting HIV”
Psychological context of ‘risk’ “Sex seems to be a primary outlet that I’ll seek whenever things get stressed” “Because I feel quite cut off with this disassociative thing Ihave got, Ifind sex is a way of feeling more engaged” “My sister died of cancer… it kind of changed my attitude towardslife and fearsand risks, because up until that point I would only have protected sex ”
PrEP for now “I want to explore this wild sex scene that cities like London or Berlin can offer… but I am beginning to lose interest … perhaps I am getting a bit bored of that” “You don’t see many 55 year old men doing group sex, clearly it is a period, a moment … it is not going to be a lifetime” “My aim would be to move to a position where I had dealt with my demons and was able to be safe, cast ironly safe, and at that stage I would be happy to not take the medication”
Conclusions In this high-risk cohort, the biological protection provided by PrEP was perceived as offering additional psychosocial benefits. PrEP was added to an existing range of 'rules' and while it impacted on the boundaries of the rules for some people, it rarely replaced them. Within the social and psychological contexts of ‘risk’, PrEP was experienced as offering increased individual choice in the mitigation of risk during periods of higher risk activity. These findings highlight the psychosocial and psychological contexts in which ‘risk’ takes place and the opportunity that PrEP provides to open up discussions about these risks.
Acknowledgements (1) Study participants MRC CTU at UCL Sarah Banbury, Liz Brodnicki, Christina Chung, Yolanda Collaco-Moraes, Monica Desai, David Dolling, David Dunn, Mitzy Gafos, Adam Gregory, Sajad Khan, Brendan Mauger, Sheena McCormack, Yinka Sowunmi, Ellen White, Gemma Wood HIV & STI Dept, PHE Monica Desai, Sarika Desai, Noel Gill, Anthony Nardone, GUMCAD team, HIV team Clinics Vanessa Apea, John Saunders, Mags Portman (Barts Health NHS Trust), Christine Bowman (Sheffield Teaching Hospitals NHS Foundation Trust), Michael Brady (Kings College Hospital NHS Foundation Trust), Martin Fisher, Amanda Clarke (Claude Nichol Centre), Julie Fox (Guy’s and St Thomas’s NHS Foundation Trust), Richard Gilson (The Mortimer Market Centre), Charles Lacey (York Hospitals NHS Foundation Trust), Nicola Mackie (St Mary’s Hospital), Alan McOwan, Simone Antonucci (56 Dean Street), Iain Reeves (Homerton University Hospital NHS Foundation Trust), Gabriel Schembri (Manchester Centre for Sexual Health), Ann Sullivan (John Hunter Clinic for Sexual Health), Steve Taylor, David White (Heart of England NHS Foundation Trust)
Acknowledgements (2) Trial Steering Committee Independent members: Mike Adler (Co-Chair), Gus Cairns (Co-Chair), Dan Clutterbuck, Rob Cookson, Claire Foreman, Stephen Nicholson, Tariq Sadiq, Matthew Williams Investigator members: Brian Gazzard, Noel Gill, Anne Johnson, Sheena McCormack, Andrew Phillips Gilead: Matt Bosse, Rich Clarke, Jim Rooney, Murad Ruf University of Liverpool: Saye Khoo Independent Data Monitoring Committee: Anton Pozniak, Simon Collins, Fiona Lampe Community Engagement Group Community: Yusef Azad (NAT), Gus Cairns (NAM), Rob Cookson (LGF), Tom Doyle (Mesmac), Justin Harbottle (THT), Marion Wadibia (NAZ), Matthew Hodson (GMFA), Cary James (THT), Roger Pebody (NAM) Clinics: Anthony Bains, Alan McOwan (Lead), MRC CTU at UCL: Sheena McCormack, Mitzy Gafos, Annabelle South Social Science Advisory Group Interviewers: Mitzy Gafos, Caroline Rae, Gill Bell, Michael Rayment, Sonali Wayal, Will Nutland Advisors: Ingrid Young, Ford Hickson, Lisa McDaid, Marsha Rosengarten, Nicolas Lorente, Agata Pacho, Elizabeth Poliquin, Anthony Nardone, Catherine Dodds, Adam Bourne, David Dolling, Sheena McCormack, Rob Horne
Poster presentation WEPEC0953 Wednesday 12:30-14:30 ”Adherence intentions, long-term adherence and HIV acquisition among PrEP users in the PROUD open-label RCT of PrEP in England”
Thank you New contact details: Mitzy Gafos STRIVE Co-Research Director London School of Hygiene and Tropical Medicine Mitzy.Gafos@lshtm.ac.uk