Download
1 / 23
310 likes | 772 Views
Endemic goiter in S ri L anka. OBJECTIVES. What is endemic goitre? Indications used to identify. Gravity of the problem How does it occur? Remedies Earlier situation in Srilanka -before 1995 Universal Salt Iodination programme-1995 Modern situation in Srilanka -after 1995

E N D
OBJECTIVES • What is endemic goitre? • Indications used to identify. • Gravity of the problem • How does it occur? • Remedies • Earlier situation in Srilanka -before 1995 • Universal Salt Iodination programme-1995 • Modern situation in Srilanka -after 1995 • Malpractices • Conclusions
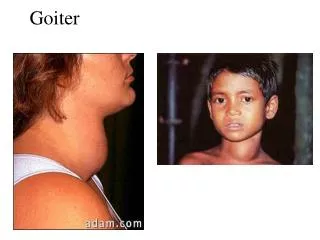
1. What is endemic goitre? • When a significant proportion of the population (over 10 %) of any region, has palpable or obviously enlarged thyroids, the condition is termed as endemic goitre.
What is endemic goitre? (continued..) • An area is considered goitrous when 5% of the girls aged 12 – 14 show clinical signs of goitre • Endemic goiter is formed in regions where the Iodine intake is less than 50 μg per day.
2. Indications used to identify endemic goitre. • The median urinary iodine(UI) level in the population ideally should be between 100 – 200 μg/L • Palpation of the thyroid gland by trained medical personnel to assess the size and shape of the gland.
3. Gravity of the problem • Affects over one billion people worldwide. • 172 million people in the south east Asia region have goitre. Further 599 million are at risk. • One of most common causes of Multi Nodular Goitreglobally. • Hypothyroidism in pregnant women can have serious adverse effects on the fetus. • Impairs genetic potential of individuals and collectively undermines the capacity of people to contribute to the development of the country.
4. How does it occur? 2 1 • Gland enlarges
How does Iodine deficiency occur? • Reduced iodine intake ( food and water) • Affects people in some geographical areasie; Mountains- central division River basin- kelani river, kalu river • Hard water consumption-Ca decrease metabolic effect of thyroxin • Goitrogens – cabbage, manioc(SCNˉ), nitrates(fertilizers)
5. Remedies Either of the following could be done as a precaution to avoid getting goitre.. • Enrichment of a common food. ie: Salt • Provision of tablets of NaI or KI. • Most common remedy is fortifying table salt with iodine.
6. Earlier to 1995 in Srilanka • The 1st of the goitre studies made in srilanka was in 1947-49 • Results suggested the existence of an endemic area for iodine deficiency (goitre belt) in srilanka. • It was confined to the south-west region of the country including western, central and southern provinces.
In other words goitre was prevalent, in the wet zone – high annual rain fall due to heavy monsoon rains . high annual rain fall was believed to leach soil iodine deficiency However, they reported that endemic goitre was not associated with cretinism to any greater extent. Ie; it was mild iodine deficiency But recent surveys have found endemic goitre in dry zone too.
Earlier to 1995 in Srilanka(continued..) • A survey done in 1989 revealed that,overall prevalence rate of goitre was 18.8% Of which 23.2% - girls and 14.0% - boys. • Prevalence in districts varied from, 6.5% in Matale to 30.2% in Kalutara • It was higher in rural than urban areas, and in inland than coastal areas.
7. Universal Salt Iodination programme-1995 • In view of these findings and parallel to the Universal Salt Iodination programme(USI), iodization of salt becoming mandatory following an enactment by the government in 1995.
Universal Salt Iodination programme-1995(continued..) • Require an iodine content of 50ppm at the factory and 25ppm at the consumer level. • Salt iodination is now used as a simple , cost effective way to prevent iodine deficiency.
8. Modern situation in Srilanka -after 1995 • The total goiter prevalence was reduced in some districts in significant levels according to the UI levels. • Nevertheless it was less than expected progress. • A research done in 2001 indicated an overall prevalence of the goitre rate was 20.9% • Although Western and Southern province goitre rates were decreased , there was a marginal in crease in Uwa and Central provinces.
Modern situation in Srilanka -after 1995(continued..) • Remarkably in the north central province(NCP) indicated more than adequate levels of urine iodine , while the total goitre rate in the NCP was among the highest in Srilanka. • Authorities still research on this to identify whether it is the Wolff-Chaikoff effect or presence of multiple goitrogensis causing this phenomenon. • Selenium deficiency in the soil is also thought to be associated with goitre prevalence.
9. Malpractices • Even the Iodine content of the iodinated salt can get lowered due to poorly monitored processes in manufacturing, transporting and storing them. • It is important to add iodized salt after cooking process as iodine could easily get destroyed by excessive heat.
10.Conclusions • Srilanka has achieved satisfactory iodine status as indicated by the UI levels.145.3 μg/L • It’s important to develop a surveillance system to monitor salt iodine content. • People should be advised properly about the goitrogens and proper use of iodinated salt.
References: • World health organization (WHO) website: www.who.int Nutrition throughout life cycle: Prof. T.W. WickramanayakeGanong’s review of medical physiology. • Research articles.
Group members • 107 - D.L. Manjula Prasad • 108 - L.G. Jeewana Prasad • 109 - D.W. Premakeerthi • 110 - T.E. Premasiri
Acknowledgment • We would like to thank Dr. Eric De Zoysa for guiding us and for the valuable support towards making this attempt a success.