Download
1 / 14
140 likes | 344 Views
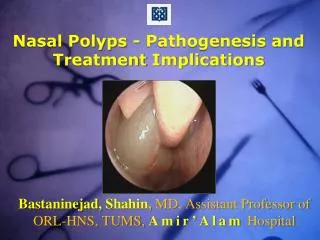
Nasal Polyps. By Alex Pearce-Smith. True of False?. More common in men? Equal gender incidence in asthmatics? More common in Afro-carribeans? Sensitive to touch? Common in children? Usually bilateral? 20% recurr after surgery?. Nasal Polyps. Background.

E N D
Nasal Polyps By Alex Pearce-Smith
True of False? • More common in men? • Equal gender incidence in asthmatics? • More common in Afro-carribeans? • Sensitive to touch? • Common in children? • Usually bilateral? • 20% recurr after surgery?
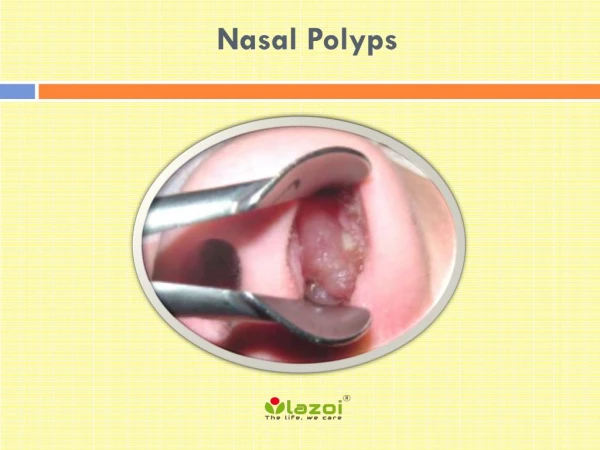
Background • Most commonly seen in middle meatus. • Eosinophil-rich oedematous wall characterised by Goblet cell hyperplasia. • Uncertain pathogenesis but linked to chronic infection and inflammation, allergy AN dysfunction and genetics. • Maybe single or multiple.
Incidence/Prevalance • Approx 2% incidence of polyps. • Rare in children and declines after 60. • Males 2-4:1 Females (except Asthma 1:1) • Prevalance – 1% adults – 0.1% children. • No racial predilection
Associations • Infective Sinusitis – Staph, Strep, Bacteroides, Pseudomonas A, • C.F. – if 16 or under consider this. Polyps found in upto 48% of children with CF. • Asthma – upto 50% prevalance. • Kartageners, Churg-Strauss, Primary ciliary diskinesia. • Not associated with Allergic Rhinitis!
Presentation • Nasal airway obstruction. • Watery Rhinorrhoea, Post-nasal drip. • Obstructive sleep symptoms/snoring. • Anosmia. • Chronic mouth breathing. • Samster’s Triad – polpys+asthma+aspirin sensitivity.
Examination • Distinguish from inferior turbinate as grey, able to get between them and the side of the nose and insensitive. • May be seen coming down into the oropharynx. • Usually Bilateral
Sinister Signs/Symptoms • Unilateral – consider cancer. • Bleeding/Crusting • Eye symptoms • Severe unilateral frontal headache. • Meningitis sx or focal neurology.
Management • Referral – unilateral, children etc. • Review associated diseases. • Education as to recurring nature. • Medical first line. • Aim of treatment is to relieve obstruction, restore olfaction, improve drainage.
Medical • Topical corticosteroids – Mometasone, Fluticasone (safe in children). NB side-effects. As nasal spray –this may be used continuously to prevent recurrence but at least 3M trial recommended) . • Step 2 – Betnesol drops – 2 drops TDS each nostril for a month (NB equiv 0.5mg prednisolone and caution in children). • http://www.derbyshirecountypct.nhs.uk/content/files/Clinical%20Guidelines/Nasal%20Polyposis%20Guideline%2005(12).pdf • Oral steroids – specialist advice.
Surgical • Alongside medical management if unsuccessful. • Either polypectomy or ethmoidectomy. • Recurrence common – 60% have repeat procedure within 5 yrs. • Less effective in patients with concurrent asthma.
True or False? • More common in men? • Equal gender incidence in asthmatics? • More common in Afro-carribeans? • Sensitive to touch? • Common in children? • Usually bilateral? • 20% recurr after surgery?