Download
1 / 105
1.14k likes | 1.57k Views
BIRTH INJURIES. DR.EJAS RAHMAN PAEDIATRICS PG 1 ST YR. DEFINITION-birth injuries. An impairment of the infant’s body function or structure due to adverse influences that occurred at birth. National Vital Statistics Report

E N D
BIRTH INJURIES DR.EJAS RAHMAN PAEDIATRICS PG 1ST YR
DEFINITION-birth injuries • An impairment of the infant’s body function or structure due to adverse influences that occurred at birth. National Vital Statistics Report • Birth injuries is defined as those injuries sustained during labour and delivery. Birth injuries may be severe enough to cause neonatal deaths, still births or number of morbidities. D C Dutta
RISK FACTORS • Primiparity • Small maternal stature • Maternal pelvic anomalies • Prolonged or unusually rapid labor • Oligohydraminos • Malpresentation of the fetus • Use of mid forceps or vacuum extraction • Versions and extraction • Very low birth weight or extreme prematurity • Fetal macrosomia or large fetal head • Fetal anomalies
PREDISPOSING FACTORS • Prolonged or obstructed labor • Fetal macrosomia • Cephalopelvicdispropotion • Abnormal presentation (breech) • Instrumental delivery • Difficult labor • Shoulder dystocia • Precipitate labor
TYPES OF BIRTH INJURIES • Soft tissue: skin- laceration, abrasions, fat necrosis. • Nerve: facial nerve, brachial plexus, spinal cord, phrenic nerve, horner’s syndrome • Eye: hemorrhages-subconjunctiva, retina • Viscera: rupture of liver, adrenal gland, spleen • Scalp: laceration, abscess, haemorrhage.
Dislocation: hip, shoulder, cervical vertebrae • Skull: cephal hematoma, subgleal hematoma, fractures • Intracranial: haemorrhages- intraventricular, subdural, subarachanoid • Bones: fractures-clavicle, humerus, femur
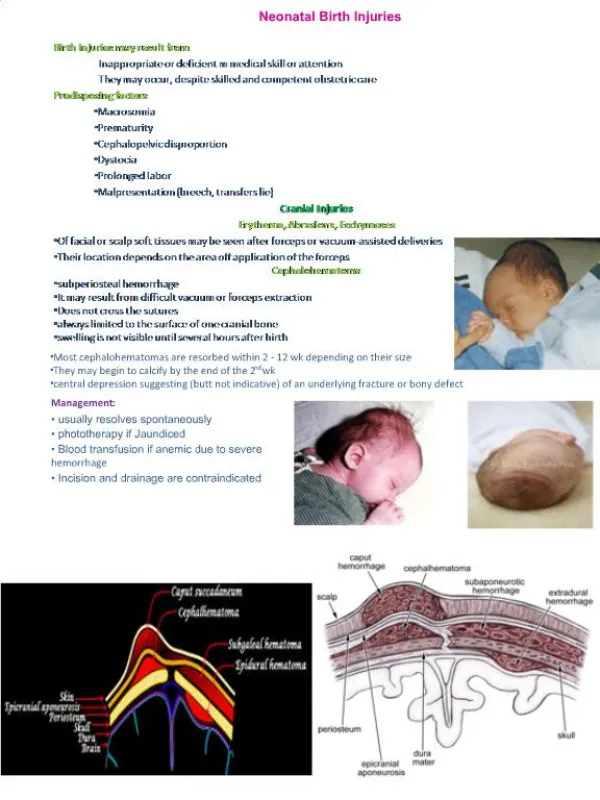
HEAD AND NECK INJURIES 1.injuries associated with intrapartum fetal monitoring 2. Extracranial hemorrhage a)Capput succedaneum b) cephalohematoma c) subgaleal hematoma 3. Intracranial haemorrhage 4. Skull fracture 5. Facial or mandibular fractures
6. Nasal injuries 7. ocular injuries 8. Ear injuries 9. Sternocleidomastoid injury 10. Pharyngeal injury
caput succedaneum: • it is a commonly occurring subcutaneous, extraperiosteal fluid collection that is occasionally hemorrhagic. • It has poorly defined margins and can extend over the midline and across suture lines. • The lesion usually resolves spontaneously without sequeale over the first several days after birth. • Vacuum caput is a caput succedaneum with margins well demarcated by the vacuum cup.
cephalohematoma It is a collection of blood between the pericranium and flat bone of the skull(subpeiosteal collection of blood), usually unilateral and over the parietal bone.
Causes • rupture of small emissary vein from the skull and may be associated with fracture of the skull bone. It is never present at birth but gradually develops after 12-24 hours. • The condition may be confused with caput succedaneum or meningocele. • Meningocele always lies over a suture line or over a fontanelle and there is impulse on crying. Prognosis is good. • Usually it resolves within 8 weeks.
subgaleal hematoma • subgaleal hematoma is hemorrhage under the aponeurosis of the scalp. It is more often seen after vaccum or forceps assisted deliveries. • the hemorrhage can spread across the entire calvarium.
Intracranial haemorrhage Traumatic: • Extraduralhaemorrhage: • Subdural: • Slight haemorrhage may occur following: • A] fracture of skullbone • B] rupture of the inferior sagital sinus • C] rupture of small veins leaving the cortex • massive haemorrhage: • a] tear of the tendoriumcerebrii • b] injury of superior sagital sinus
mechanism of tentorial tear: • normally falxcerebri attached to the tentoriumcerebri and both anchoring the base of the skull to the vault. • This results in the upward movement of the vault from the base. • As a result, too much strain is put on the vertical fibres of tentorium cerebella- called stress fibres. • If the moulding is excessive or applied suddenly, these fibres are torn. • as a result it allows excessive elongation of the vault until the tear extends to involve the straight sinus or vein of Galen or its tributaries.
Causes • excessive moulding in deflexed vertex with gross disproportion. • Rapid compression of the head during the delivery of after coming head of breech or in precipitate labor. • Forcible forceps traction following wrong application of the blades.
Clinical features • The hemorrhage may be fatal • the baby is delivered stillborn or with severe respiratory depression having an apgar score 0-3. • The features cerebral irritation include frequent high pitch cry, neck retraction, in-coordinate ocular movements, convulsions, vomiting and bulging of anterior fontanelle.
Anoxic: • Intraventricular • Subarachanoid. • Intracerebral.
PREVENTION • Prevent or to detect earliest, intrauterine fetal asphyxia • Avoid traumatic vaginal delivery. • Extend the use of caesarean section in breech more liberally. • Administration of vitamin K 1 mg intramuscularly soon after birth
INVESTIGATIONS: • Ultrasongraphy used to detect intraventricular hemorrhage • Doppler ultrasonography to detect any change in the cerebral circulation. • CT scan is useful to detect cortical neuronal injury. • MRI used to identify hypoxic ischemic brain injury. • CSF: hemorrahage
TREATMENT • The baby should be nursed in quite surroundings. • Incubator nursery is preferable to supply oxygen and to maintain the temperature and humidity. • To maintain cleanliness of the air passages. • To maintain normal range of PaCO2 and to avoid hypoxemia • To restrict handling the baby, as such bathing, weighing and measuring should be withheld.
Feeding by nasogastric tube is advisable. Fluid balance is to be maintained, if necessary by parenteral route. • To administer vitamin K 1 mg intramuscularly to prevent further bleeding due to hypoprothrobinemia. • Prophylactic antibiotics is to be administered. • Anticonvulsants: phenobarbitone 5-10 mg/kg/day in divide doses at 6 hourly intervals intramuscularly, phenytoin 10-15 mg/kg/day with cardiac monitoring • Subdural tap for subdural hematoma
Skull fracture • Fracture of the vault of the skull may be fissure or depressed type. • Fractures are due to • Effect of difficult forceps in disproportion or due to wrong application of the fo4rceps. • Projected sacral promontory of the flat pelvis may produce depressed fracture even though the delivery is spontaneous.
Facial or mandibular fractures • Facial fractures can be caused by numerous forces, including natural passage through the birth canal, forceps use or delivery of the head in breech presentation.
Nasal injuries • Nasal fracture and dislocation may occur during the birth process. The most frequent nasal injury is dislocation of the nasal cartilage, which may result from pressure applied by the maternal symphysis pubis or sacral promontory.
ocular injuries • They result from increased venous congestion and pressure during delivery. Retinal hemorrhages usually resolve within 1 to 5 days. Sub-conjunctival hemorrhages reabsorb within 1 to 2 weeks.
Ear injuries • Ears are susceptible to injury particularly with forceps application. More significant injuries occurs with fetal malposition. • Hematomas of the ear may lead to development of a “cauliflower” ear.
Sternocleidomastoid injury • referred to as congenital or muscular torticollis. The etiology is uncertain. The most likely cause is a muscular compartment syndrome resulting from intrauterine positioning.
It may present at birth with a palpable 1 to 2 cm mass in the SCM and head tilt to the side of the lesion. • Treatment is usually conservative. Stretching of the involved muscle should begin promptly and be performed several times per day. • Surgery needed if it persists after 6months of physiotherapy.
Pharyngeal injury • Minor submucosal pharyngeal injuries can occur with postpartum bulb suctioning. More serious injury, such as perforation into the mediastinal or pleural cavity, may result from nasogastric or endotracheal tube placement.
CRANIAL NERVE, SPINAL CORD AND PERIPHERAL NERVE INJURY Cranial nerve injury • Facial nerve injury: • Recurrent laryngeal injury spinal cord injuries Vaginal delivery of an infant with a hyper extended neck or head, breech delivery and severe shoulder dystocia are risk factors for spinal cord injury. Injuries include spinal epidural hematomas, vertebral artery injuries, traumatic cervical hematomyelia, spinal artery occlusion and transaction of the cord.
cervical nerve root injury • Phrenic nerve injury Phrenic nerve damage leading to paralysis of ipsilateral diaphragm may result from a stretch injury due to lateral hyper extension of the neck at birth. Risk factors include breech and difficult forceps deliveries.
Brachial plexus injury • The cause is excessive traction on the head, neck and arm during birth.the risk factors include shoulder dystocia, macrosomia, malpresentation and instrumented deliveries.
Duchenne- Erb palsy involves the upper trunks (C5, C6 and occasionally C7) and is the most common type of brachial plexus injury. The arm is typically adducted and internally rotated at the shoulder. There is extension and pronation at the elbow and flexion of the wrist and fingers in the characteristics “waiter’s tip” posture.the deltoid, infraspinatus ,biceps, supinatior and brachioradialis muscles and the extensors of the wrist and the fingers may be weak or paralysed. The moro, biceps, and the radial reflexes are absent on the affected side. Diaphragm paralysi occurs in 5% of cases.
Total brachial plexus injury accounts for approximately10% of all cases. The entire arm is flaccid. All reflexes including grasp and sensation, are absent. If sympathetic fibres are injured at T1, Horner syndrome may be seen.
Klumpke palsy- therarest of the palsies accounting for <1% of brachial plexus injuries. The lower arm paralysis affects the intrinsic muscles of the hand and the long flexors of the wrist and fingers. The grasp reflex is absent. However, the biceps and radial reflexes are present. There is sensory impairment on the ulnar side of the forearm and the hand. Because the first thoracic root is actually injured, its sympathetic fibres are damaged, leading to an ipsilateral Horner syndrome.
BONE INJURIES • clavicular fracture These fractures are seen in vertex presentations with shoulder dystocia or in breech deliveries when the arms are extended
long bone injuries • Humeral fractures typically occur during adifficulty delivery of the arms in the breech presentation and/ or of the shoulder in vertex. Direct pressure on the humerus may also result in fracture. • Femoral fractures usually follow a breech delivery. Infants with congenital hypotonia are at increased risk. Physical examination usually reveals an obvious deformity of the thigh
INTRA ABDOMINAL INJURIES • Hepatic injury • Splenic injury • Adrenal hemorrhage
SOFT TISSUE INJURIES • petechiae and ecchymoses The birth history, location of lesions, they are earely appearance without development of new lesions, and the absence of bleeding from other sites help to differentiate petechiae and ecchymoses secondary to birth trauma from those caused by a vasculitis or coagulation disorder.
Most ecchymoses and petichae resolve with in 1 week. • If bruising is excessive, jaundice and anaemia may develop. • Treatment is supportive.
lacerations and abrasions It may be secondary to scalp electrodes and fetal scalp blood sampling or injury during birth. Deep wound(eg. Scalpel injuries during cesarean section) may require sutures. Infection is a risk particularly with scalp lesions and an underlying caput succedaneum or hematoma. Treatment includes cleansing the wound and close observation.
Subcutaneous fat necrosis It is not usually recognized at birth. It usually presents during the first 2 weeks after birth as sharply demarcated; irregularly shaped; firm and non pitting subcutaneous plaques or nodules on the extremities, face, trunk or buttocks. The injury may be colorless or have a deep red or purple discoloration. Calcification may occur. No treatment is necessary. Lesions typically resolve completely over several weeks to months.
PREVENTION OF INJURIES IN NEWBORN ANTENATAL PERIOD • To screen out the at risk babies likely to be traumatized during vaginal delivery and to employ liberal use of elective CS. Contracted pelvis and CPD or malpresentation like breech or transverse lie are included in the list
INTRANATAL PERIOD • Normal delivery • continous fetal monitoring to prevent traumatic cerebral anoxia • episotomy should be done carefully • the neck should not be unduly strechted while delivering the shoulder to prevent injuries to the brachial plexus or sternomastoid. • Special care to the preterm to prevent anoxia, avoid strong sedatives, liberal episiotomy and to administer Vit K 1mg IM to prevent haemorrhage from the traumatized site.
Forceps delivery • Difficult forceps are to be avoided in preference to the safer CS. • Never apply traction unless the application is a correct one. Ventouse delivery • It is relatively less traumatic. But it should be avoided in preterm. Vaginal breech delivery • Proper selection of cases and utmost care and gentleness are to be executed while conducting breech delivery. Most crucial period of breech delivery is the delivery of the after coming head.
ENTERO HEPATIC CIRCULATION AND NORMAL BILIRUBIN METABOLISM IN A NEWBORN • 1. Source of production: Bilirubin is derived from the breakdown of hemeproteins which are present in hemoglobin, myoglobin and certain heme containing enzymes. Three fourths of the bilirubin comes from hemoglobin catabolism. One gram of hemoglobin results in the production of 34 mg of bilirubin. A normal term newborn produces about 6-10 mg/kg/ day of bilirubin.