Download
1 / 52
590 likes | 973 Views
Surgical treatment of t uberculosis (TB). Department of Thoracic Surgery, General and Oncological Surgery. EPIDEMIOLOGY. Tuberculosis (TB) is an infectious disease caused by acid-fast strains of mycobacteria, (Mycobacterium tuberculosis), which was discovered by Robert Koch in 1882.

E N D
Surgical treatment of tuberculosis (TB) Department of Thoracic Surgery, General and Oncological Surgery
EPIDEMIOLOGY • Tuberculosis (TB) is an infectious disease caused by acid-fast strains of mycobacteria, (Mycobacterium tuberculosis), which was discovered by Robert Koch in 1882. • It is estimated that one third of world population is suffering from TB and nearly half of new TB patients come from south Asia. • TB incidence is reported for 8-9 million new patients a year.
EPIDEMIOLOGY • TB mortality is estimated for 3 million a year. • Despite the presence of highly efficient antitubercular drugs TB incidence rate is on increase since the beginning of 1985.
EPIDEMIOLOGYThe main reasons for that are as follows: • deteriorating social conditions • intravenous drug injections • limited access to public health service • secondary resistance to treatment of mycobacteria • immunosuppression in the course of diseases such as AIDS • systemic chemiotherapy
EPIDEMIOLOGY • In Poland the incidence rate is on the decrease. In the 50s of the previous century TB was diagnosed in 20% of the population. • At present, each year TB afflicts nearly 100.000 people in Poland • The most endangered are elderly people (65 years old and more)
EPIDEMIOLOGY • The most common site of TB infection are lungs. • In case of normally functioning immune response TB infection is asymptomatic • Only 10% of TB infections result with development of the disease • Approximately 5% of people develop primary TB, directly after the infection. • Others are likely to develop TB many years after infection due to TB reactivation (post-primary TB).
SYMPTOMATOLOGY • The most common TB symptom is prolonged cough (lasting over 3 weeks)-first dry (non-productive), then moist (productive) cough with mucopurulent sputum
SYMPTOMATOLOGY Moreover some nonspecific symptoms can be observed such as: • fatigue, • weakness, • weight loss, • night sweats, • low-grade fever • dyspnoea (is usually present in advanced stages of TB infection).
SYMPTOMATOLOGY • Physical examination reveals no specific signs. • Chest percussion may detect a dullness over the affected area • Auscultation usually detects silenced vesicular respiration as a result of atelectasis or pulmonary infiltration.
SYMPTOMATOLOGY • In primary TB chest X-ray may reveal condensations located in the middle or upper lung fields. • Typical X-ray signs of TB include: • patchy infiltrates, • cavity formation, • scar tissue, • calcium deposits, however, it may not be able to distinguish active from inactive TB.
SYMPTOMATOLOGY • In 30% of TB cases nodular enlargement in the hili and near trachea (mainly right-sided) is observed. • Significant nodular enlargement may result in atelectasis, oesophageal compression or superior caval vein syndrome. • In 15% of TB cases regular chest X-ray reveals no abnormalities!
SYMPTOMATOLOGY Post-primary TB is characterized by condensations located in apical lobes and upper posterior lobes. TB infiltrates may be absorbed or heal by fibrosis.
DIAGNOSTICS • To confirm TB suspicion, smears and cultures must be collected (sputum, CSF, urine, drainage from abscess or pleural fluid). • In some patients microscopic examination (Ziehl-Neelsen’s staining or fluorescent staining methods) shows the presence of tubercle bacilli (“open” active TB).
DIAGNOSTICS • Conventional methods of TB diagnostics may take up to 4 months: repeated bacteriological cultures- if positive confirm TB diagnosis, negative- have no exclusive power). • The most recent methods include: • BACTEC (marked fatty acids detection) -results after 1-2 weeks • Mycobacterium DNA detection (PCR method) -1 week.
PHARMACOLOGICAL TREATMENT • Pharmacological treatment of TB is divided into two phases: -introductory (usually 2 monthsmulti-drug therapy: INH+RMP+PZA+EMB) -maintaining phase (4 months: INH+RMP).
PHARMACOLOGICAL TREATMENT • The treatment usually takes 6 months (9 months in AIDS patients). • Antitubercular therapy involves: -INH(isoniazid), -RMP (rifampicin), -EMB (etambulol), -SM (streptomycin), -PZA (pyrazinamide).
HISTORY OF SURGICAL TREATMENT OF TB In 1882 Forlanini and in 1889 Murphy performed intrapleural pneumothorax in TB treatment as the immobilized part of the lung with TB was expected to heal faster.
HISTORY OF SURGICAL TREATMENT OF TB • Other methods of surgical treatment of TB involved: -pneumoperitoneum (aeroperitoneum), -phrenoplegia (phrenic nerveparalysis), -extrapleural pneumothorax (surgical emphysema).
HISTORY OF SURGICAL TREATMENT OF TB • Despite many therapeutic advantages of aforesaid surgical methods in TB treatment, they were endangered with many possible complications such as: •Thoracic emphyema (pyothorax) •Bronchopleural fistula •Haemorrhage •Translocation of materials used in artificial pneumothorax creation to other body’s cavities
HISTORY OF SURGICAL TREATMENT OF TB • Another method that led to pulmonary collapse in TB treatment was resection of ribs (so called thoracoplasty). • It was first performed by Eduard de Carneville in 1885.
HISTORY OF SURGICAL TREATMENT OF TB • First pulmonectomy was conducted by Block in 1882, but turned out unsuccessful. • Finally, successful pulmonary resection took place in 1891 (Tuffier).
HISTORY OF SURGICAL TREATMENT OF TB • Full-scale pulmonary resections were conducted in the 30s of the 20th century. • The problematic issue was, however, the Turniekitov method of surgical supply of pulmonary hilus „en block” without preparation of particular anatomic elements!
HISTORY OF SURGICAL TREATMENT OF TB • This resulted in high postoperative complications rate, that reached 20%after lobectomy and 40% after pulmonectomy.
HISTORY OF SURGICAL TREATMENT OF TB • In the 40s and 50s more tuberculostatic drugs were introduced into clinical practice and surgical techniques got improved- both resulted in better outcomes of surgical treatment of TB.
HISTORY OF PHARMACOLOGICAL TREATMENT OF TB • The first effective antitubercular drug was streptomycin, which was discovered by Waksman and introduced to clinical practice in 1945. • In 1946 para-aminosalicylic acid and in 1951 isoniazid (INH) were introduced to antitubercular therapy.
HISTORY OF PHARMACOLOGICAL TREATMENT OF TB • Since then the number of medicaments in TB treatment have grown rapidly, which resulted in diminishing of indications for surgical treatment of TB.
SURGICAL TREATMENT OF TB The role of surgical treatment in TB is inversely proportional to conservative therapy!!!
SURGICAL TREATMENT OF TB The surgical techniques in TB treatment comprise: •Pulmonary segment resection(segmentectomy) with/without thoracoplasty •Pulmonary lobe resection (lobectomy) with/without thoracoplasty •Pulmonectomy with thoracoplasty
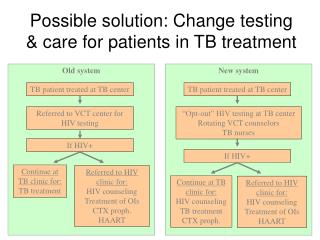
SURGICAL TREATMENT OF TB Nowadays in clinical practice there are 2 indications for surgical treatment in TB: • Ineffective antitubercular therapy and sputum-positivity that remains 12 months after pharmacological treatment • Tuberculous complications, that can be treated only with surgical methods
SURGICAL TREATMENT OF TB Absolute indications The most common reasons for ineffectiveness of antitubercular therapy and sputum-positivity after 12 months of pharmacotherapy are: •Atypical mycobacteria •Mycobacterial resistance to antitubercular drugs •Contraindications to conventional antitubercular treatment •Non-compliance of TB patient •Other, less known reasons
SURGICAL TREATMENT OF TB Absolute indications TB complications, that can be treated only with surgical methods: •Pulmonary bleeding or haemorrhage •Pyothorax with or without bronchopleural fistula (that could not be treated conservatively) •Tubercular cavity’s superinfection (aspergillosis) •Bronchostenosis in patients who underwent nodulo-bronchial TB
SURGICAL TREATMENT OF TB Relative indications Persistent tuberculous cavity- arguments in favour of surgical treatment: •High risk of TB recurrence •High risk of superinfection (aspergillosis) •The risk of bleedings •The risk of bronchopleural fistula formation •The risk of pyothorax formation
SURGICAL TREATMENT OF TB Relative indications •Round shadows in the lungs (tuberculoma, caseous TB) In such cases surgical treatment is recommended due to: -diagnostic problems in defining the ethiology of round shadows in the lungs (surgery is considered better solution in comparison to neoplastic process omission) -poor penetration of antitubercular drugs to TB cavities (poor blood supply of the capsule)
SURGICAL TREATMENT OF TB Relative indications When the lung is destroyed by tuberculous process, surgery is recommended in case of: •High risk of TB recurrence •High risk of aspergillosis, pyothorax and bleedings •The shunt of unoxigenated blood from destroyed lung to the healthy one
SURGICAL TREATMENT OF TB Relative indications The opponents of surgical treatment consider surgery as necessity only in case of TB recurrence or TB complications.
SURGICAL TREATMENT OF TB Contraindications to surgical treatment •Respiratory system insufficiency -VC< 1,1 or < 50% of reference value -FEV1< 0,9 or < 50% of -PaO2 < 55mmHg and PaCO2 > 45mmHg •Cardiovascular insufficiency or/and renal failure(hypouresis, increase of serum creatinine, ureaand kalium levels)
SURGICAL TREATMENT OF TB Contraindications to surgical treatment • Extent of TB infiltrates in lungs -bilateral and affecting two lobes each side. Exceptions are: micromacular and fibrous TB infiltrates without features of decay unilaterally and in case of tuberculous infiltrates affecting one lobe each side when spirometric values are satisfactory (one-stage or two-stage surgery can be performed in such cases)
SURGICAL TREATMENT OF TB Contraindications to surgical treatment • Patient’s age – there are no absolute criteria. The most important is evaluation of general condition and evident advantages of surgical treatment in particular patient
SURGICAL TREATMENT OF TB • During the surgery, prevention of pleural cavity infection is crucial. • The incision should be performed within healthy tissues, as the surgery aims at removing the infiltrated lung’s part „en bloc”. • After the excision it is necessary to apply pleural drainage.
SURGICAL TREATMENT OF TB Postoperative management involves: • prevention of atelectasis • fluid balance control • if necessary -administration of blood, -packed RBCs, -fresh-frozen plasma to support hemostasis.
SURGICAL TREATMENT OF TB Postoperative complications comprise: -bleedings -atelectasis -lung fibrosis -pyothorax -pulmonary embolism -bronchopleural fistula