Download
1 / 22
300 likes | 1.06k Views
THROMBOLYTIC DRUGS Pathophysiologic Rationale. When an atherosclerotic plaque ruptures thrombosis occlusion of the artery myocardial infarction necrosis If we can breakdown the thrombus then we can save the myocardial cells from necrosis.

E N D
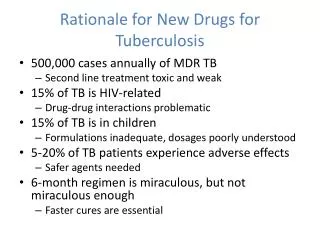
THROMBOLYTIC DRUGSPathophysiologic Rationale • When an atherosclerotic plaque ruptures thrombosis occlusion of the artery myocardial infarction necrosis • If we can breakdown the thrombus then we can save the myocardial cells from necrosis. • Clinical trials of thrombolytic drugs showed beneficial in patient with MI with ST segment elevation. • But they weren’t as beneficial when it came to unstable angina or MI with non ST segment elevation • The treatment should be initiated rapidly (less than 6 hours)
Fibrinolysis TPA: tissue plasminogen activator
Mechanism of Thrombolytic Drugs • They convert plasminogen plasmin which lyses blood clots • Plasmin, is a nonspecificserine protease(capable of breaking down fibrin as well as fibrinogen (main action)and factors V and VIII)
Mechanism of Thrombolytic Drugs • The plasmin(ogen) molecule has lysine binding sites, which bind to fibrin $2200 $280 prodrug Secreted from kidney
I- Streptokinase (SK) • It is a bacterialprotein (not an enzyme)produced by group C β-hemolytic streptococci. SK activator complex (SK+plasminogen) Plasminogen Activator complex Plasminogen Plasmin Lysis of fibrin clot N.B. Plasmin degrades fibrin clots as well as fibrinogen and other plasma proteins (non-fibrin specific)
Cont’d activate degrade
Cont’d • Pharmacokinetics: • The t½ of the activator complex= 23 minutes • The complex is inactivated by anti-streptococcal antibodies & by hepatic clearance • It produces hyperfibrinolytic effect, which decreases plasma fibrinogen levels for 24-36 hrs • A prolonged bleeding time may persist for up to 24 hours due to the decrease in plasma levels of fibrinogen
Cont’d • Efficacy: reduces mortality: • 47 % reduction after one hour of chest pain. • 23% within 3 hours • 17% between 3-6 hours • No significant reduction between 6-12 hours • Hospital cost per day is minimal 280 $ • The advantages are more when take rapidly (at the onset of chest pain)
Cont’d • Clinical Uses: • Acute Myocardial Infarction: administered IV or intracoronary ↓ infarct size and congestive heart failure. • Arterial Thrombosis or Embolism: It is not indicated for arterial emboli originating from the left side of the heart due to the risk of new embolic phenomena such as cerebral embolism. • Occlusion of Arteriovenous Cannulae: for clearing totally or partially occluded arteriovenous cannulae.
Cont’d • Side-Effects: • Bleeding due to activation of circulating plasminogen • Hypersensitivity: because it is of bacterial products so, it is antigenic & can produce allergic reactions like rashes & fever (occurs in 3% of patients)
II- Anistreplase (APSAC) • Anisoylated Plasminogen Streptokinase Activator Complex (APSAC) purified human plasminogen combined with bacterial streptokinase that has been acylated to protect the enzyme’s active site. • It is a prodrug: APSAC SK-plasminogen complex • Similar to SK, it has minimal fibrin specificity & is antigenic • T1/2 is more than SK (70-120 min ) • Hospital cost per day is 1700 $ deacylation
III-Alteplase (rt.PA) • Formerly known as tissue plasminogen activator (t-PA). • Mechanism of action: • It is an enzyme. • rt.PA binds to fibrin conversion of plasminogen to plasmin (inside the clot) fibrinolysis • It acts only on fibrin inside the clot (not free fibrin) It’s fibrin selective (specific)
cont’d • Pharmacokinetics: t1/2 = 5 minutes • produced by recombinant DNA technology. • Cost per day is around 2200 $ (expensive)
Cont’d Therapeutic Uses • Acute Myocardial Infarction: • Reduces mortality • Improve ventricular function ↓ CHF • Acute Ischemic Stroke • improves neurological recovery • reduces the incidence of disability. • Treatment of acute massive Embolism • Treatment should only be initiated within 3 hours after the onset of stroke symptoms. • You have to exclude cerebral hemorrhage to use alteplase (see adverse effect in the next slide)
Cont’d • Side-Effects: • Bleeding including GIT & cerebral hemorrhage • Allergic reactions: rare (< 0.02% of patients) (minor effect)
IV-Urokinase • It is an enzyme produced by the kidney of human & also animal ( yet no allergic reaction) and is found in urine. • It is mainly used in the low molecular weight form of urokinase obtained from human neonatal kidney cells grown in tissue culture. • Mechanism: It acts on the endogenous fibrinolytic system converting plasminogen to plasmin that degrades fibrin clots as well as fibrinogen and some other plasma proteins (Non-fibrin selective).
Cont’d • (IV) administration • rapidly cleared by the liver • t1/2 = 12-20 minutes Clinical Uses: • For the lyses of acute massive pulmonary emboli Pharmacokinetics
Cont’d Contraindications to Thrombolytic Therapy
Fibrinolytic Inhibitors • Aminocaproic Acid & tranexamic acid • They have lysine-like structure • They inhibit fibrinolysis by competitive inhibition of plasminogen activation • ِِِAdjuvant therapy in hemophilia, fibrinolytic therapy-induced bleeding & postsurgical bleeding • Aprotinin is a serine protease inhibitor • It inhibits fibrinolysis by blocking free plasmin • Used to stop bleeding in some surgical procedures
ZuBDAS, in other words: (butter of the lecture) 1- All thrombolytic drugs cannot be used in case of unstable angina (could mobilize the thrombus embolism) 2- All thrombolytic drugs can be used in case of acute MI (more effective in the first 6 hours). 3- SK & Anistriplase have same MOA, ADR & selectivity. The only difference between them is that the anistriplase has relatively longer duration of action. 4- All thrombolytic drugs are non-selective except Alteplase. 5- All thrombolytic drugs have short duration of action except anistreplase (relatively) 6- All non-selective thrombolytic drugs cause more bleeding tendency than selective. Yet in general all cause bleeding 7-Streptokinase may cause hypersensitivity reaction 8-Urokinase is used primarily in pulmonary embolism treatment