Download
1 / 30
420 likes | 786 Views
Duchenne’s Muscular Dystrophy: A Multidisciplinary Approach. By: Brittany Annis, Student PT Ithaca College 2010. Objectives. Introduce background information on Duchenne’s Muscular Dystrophy Identify associated pathologies

E N D
Duchenne’s Muscular Dystrophy:A Multidisciplinary Approach By: Brittany Annis, Student PT Ithaca College 2010
Objectives • Introduce background information on Duchenne’s Muscular Dystrophy • Identify associated pathologies • Identify and explain the benefits of the multidisciplinary team members • Describe the goals and interventions of physical therapy for DMD • Describe current evidence and recommendations for exercise and DMD
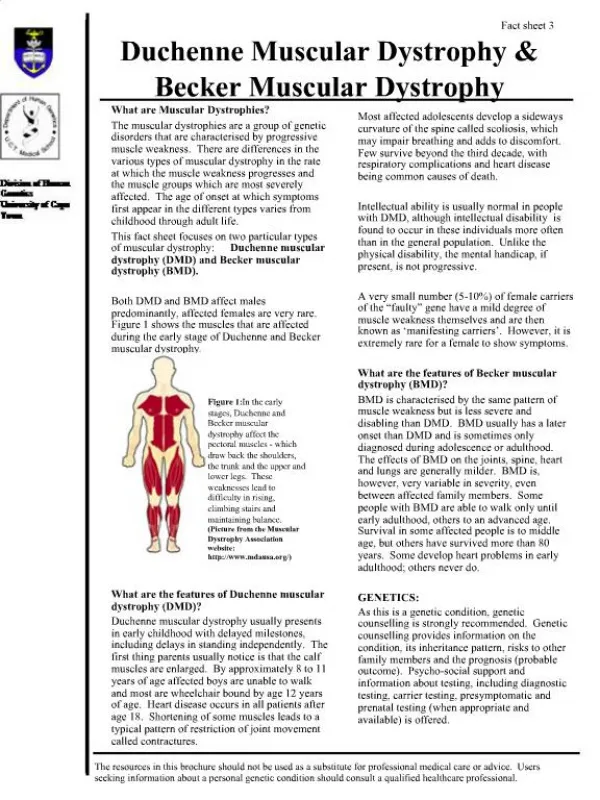
Intro to DMD • Most prevalent childhood muscular dystrophy, every 1 in 3000-6000 male births • X-linked recessive disorder- gene deletion • Deficiency of the muscle protein Dystrophin • Progressive muscle weakness in skeletal, smooth, and cardiac muscle • It has been observed that there is a greater number of Type II muscle fibers with degeneration compared to Type I.
Dystrophin • Provides mechanical reinforcement to the sarcolemmal membrane of muscle fibers; protects muscle fibers from being damaged while stressed during muscle contraction.
Lifespan of DMD • Shortened lifespan due to progressive muscle weakness and complications- mean age is 19 without intervention, mid-to-late twenties with proper care. • Now, studies and research are showing that if properly diagnosed, individuals with DMD can have possible lifespan into their forties
Signs and Symptoms • Early signs between ages 3 and 5, when most commonly diagnosed • Delayed walking • Inability to run, jump, keep up with peers • Difficulty climbing stairs • Gower’s Sign • Frequent falls • Occasionally (30%) global developmental delay and delayed speech
Associated Pathologies: Weakness • Progressive weakness of hip and shoulder girdle musculature • Weakness in paraspinals make walking difficult • Leads to: • Waddling gait • Lumbar lordosis • Forward thrusting of the abdomen • Scapular winging • Anteroposterior scoliotic curve • Joint contractures • Respiratory impairment • Weight gain
Mainly found at hips, knees, ankles Contractured Tensor Fascia Latae: Waddling gait Tightened IT Band Resultant hip and knee pain/deformities Equinovarus: Ankle plantarflexion and supination Tight gastrocnemius mm/Achilles tendon Associated weakness of tibialis anterior and peroneal mms Complications include: Difficulty wearing shoes Foot pain Hypersensitivity Concern about foot’s appearance Associated Pathologies: Joint Contractures
Associated Pathologies:Scoliosis • Most commonly seen when non-ambulatory, due to increased amount of time spend seated in a wheelchair • May require spinal fusion to promote better sitting and comfort, to prevent further deformity, avoid respiratory compromise
Can alter the natural progression of the disease and improve function and quality of life. Comprehensive set of recommendations to manage the wide spectrum of complications Includes: Rehabilitation Orthopedics Pharmocologics Psychosocial Respiratory care Cardiovascular care Pain Gastroenterology/ Nutrition The Multidisciplinary Team
Corticosteroids • Currently the best treatment option available • Improve muscle strength and function • Significantly slow the progression of muscle weakness • Prolong ambulation to mid-teens or later • Delay the onset of respiratory and/or cardiac dysfunction • [Use caution: complications include weight gain, vertebral fractures, failure to gain height, irritability]
Respiratory Management • Patients with DMD are at increased risk of respiratory complications • Because of progressive loss of muscle strength: • Cough may be ineffective • Nocturnal hypoventilation • Sleep-disordered breathing • PT can assist with respiratory management by having patient breathe against a resistive load (water in pool), breath-holding, bubble-blowing, to improve ventilatory strength and endurance. • Important to note signs and symptoms of hypoventilation to refer patient to respiratory physician. • Fatigue, dyspnea, tachycardia, morning/continuous headaches, sleep dysfunction, nightmares, difficulty concentrating
Cardiac Management • Cardiomyopathy and/or cardiac arrhythmia are major sources of mortality in DMD • The heart/myocardium have areas of hypertrophy, atrophy, and fibrosis • Failure to see a cardiac specialist early in the disease process have led to late treatment and poor outcomes • Higher levels of fitness are associated with better cardiac health
Potential Surgeries • Heelcord lengthening • Hamstring lengthening • ITB lengthening • Cannot perform hip flexor lengthening (responds poorly, weakens muscles and cannot properly brace) • Hip deformities often correct themselves once knee and ankle malalignments have been altered. • Surgery in the late ambulatory phase or after is usually not effective.
Other Important Teams: • Nutritional, swallowing, gastrointestinal, speech and language, pain management, psychosocial, pharmacological • All fields are continuously changing as the stages of the disease change
Goals of Physical Therapy • Prolong independent ambulation • Maximize functional ability • Prevent complications of inactivity • Improve emotional well-being
Stretching/Positioning Management of contractures Assistive devices Exercise Objective measures and testing to monitor progression Physical Therapy Interventions
Strength testing- MMT to monitor disease progression and predict functional losses, assess responses to treatment and monitor muscle imbalances Test LEs every 6 months when ambulatory; test UE and LE every 6 months when non-ambulatory ROM: goniometry to identify hypomobility, jt contractures that may contribute to functional deterioration or to musculoskeletal/integumentary complications, or to note need of splinting/orthotics. In ambulatory phase, measure hips, knees, ankles (ITB, H/S, heelcords). In non-ambulatory phase, measure UE as well as LE (elbows, wrists, finger flexors) Objective Measures
Timed Testing: Standardized tests are responsive to change, easy to administer, relevant to function (when ambulatory only) Timed 10 meter walk, timed Gower’s manuever, time to climb 4 stairs, 6 min walk test ADLs: Assessment of impairment in home, school, community settings Frequency of falls, self-care skills Objective Measures, Con’t
Combination of AROM, AAROM, PROM, prolonged elongation (splinting, positioning) Minimum of 4-6 days per week, at home/school and in the clinic Heelcords: Gastrocnemius/ Achilles Tendon lengthening into dorsiflexion Tensor Fascia Latae/Iliotibial Band: stretch hip into adduction, internal rotation, and extension. Other muscles throughout the hips, knees and ankles In non-ambulatory phase, also focus on upper extremities: finger flexors, wrist flexors, elbow and shoulder joints Stretching
Assistive Devices: AFOs • Custom-molded and comfortable for optimum foot and ankle alignment • Throughout life: AFO’s are appropriate at night to prevent or minimize the progression of equinus contractures • Late stages: • KAFOs for non-ambulatory boys to prevent contracture and deformity (not for use at night) • Resting hand splints for finger flexors
Wheelchair: Need appropriate postural positioning to prevent scoliosis and back pain/aches Powered for more involved patients. Manual Lightweight for less involved patients so can self propel and increase independence, as well as provide arm exercise Standing Frames: A few hours per day, even with minimal weight bearing, to prevent and reduce the severity of contractures, decubitis ulcers, and scoliosis. Also improves bone mineral density, circulation, and GI and respiratory functions. Assistive Devices Con’t
Exercise • There is a high level of controversy concerning whether exercise is beneficial or harmful to patients with DMD • Normal, dystrophic muscle (those without muscular dystrophy) can withstand mechanical forces during contraction. • Those with muscular dystrophy are compromised due to weakened muscles, joints, tendons, and bones during muscle contractions and weight-bearing. • But exercise is very important to avoid disuse atrophy and other secondary complications of inactivity
Type I muscle fibers are slow twitch for slower contractions, and fatigue-resistant, so good for continuous contractions (postural muscles) Type II muscle fibers are fast twitch for quick contractions, and are easily fatigued (“sprinter” muscles). They are also less resistant to mechanical stresses (more easily injured) It is possible to switch Type II muscle fibers to Type I with exercise training, so with an increased number of Type I fibers, the muscles are more durable and more resistant to degeneration. But the form of exercise needed to switch Type II fibers to Type I is very specific Type I vs Type II Fibers
In a mouse study, a greater percentage of Type I muscle fibers were observed after low intensity, long-term exercise Sedentary mice with DMD had a higher percentage of Type I fibers than sedentary mice without DMD It has been observed that Type II muscle fibers are subject to greater degeneration, and the majority of research using animal models and some human studies suggest that increasing activity may actually slow the degeneration in dystrophic muscle. Current Evidence Regarding Exercise
Current Evidence, Con’t • Further studies and information are needed for each subtype of muscular dystrophy to create subtype-specific recommendations, including specifics such as age, severity, rate of progression, and level of motivation.
Low resistive and aerobic exercise are justified to: Prevent deconditioning, decreased fitness, disuse atrophy and joint contractures Counteract secondary complications of inactivity such as obesity, Diabetes, osteoporosis and cardiovascular diseases Long term, low-intensity, preferably no load (or low-load) weight-bearing activity to reduce mechanical stress on the muscle Increased Type I fibers, which are less vulnerable to degeneration Will not promote hypertrophy Recommended Exercise for DMD
Use caution to ensure that cardiovascular or muscular complications do not develop High-resistance and eccentric exercise is NOT recommended, although it has not actually been proven harmful for a DMD patient Aquatic Therapy! Excellent for improving/ maintaining mobility, strength, flexibility, and aerobic conditioning and cardiopulmonary fitness Recommended Exercise for DMD, Con’t
Current Evidence • Research and studies are being done with continuous advances and milestones in DMD research • The severity of DMD can be determined by a positive correlation to the amount of dystrophin present in the muscle (the more dystrophin, the less severe the symptoms and progression) • Corticosteroid prednisone was found effective in slowing the progression of DMD, and it also stimulates utrophin production ( a mm protein similar to dystrophin) • Gene therapy clinical trials are underway and dystrophin gene injections are judged safe in clinical trial including 6 boys with DMD; studies are being continued
Works Cited Ansved, Tor. "Muscular Dystrophies: Influence of Physical Conditioning on Disease Evolution." Current Opinion in Clinical Nutrition and Metabolic Care 6 (2003): 435-39. Print. Bushby, Katharine, Richard Finkel, and David Birnkrant. "Diagnosis and Management of Duchenne Muscular Dystrophy, Part 1: diagnosis, and pharmacological and psychosocial management." 30 Nov. 2009. Web. 1 Dec. 2009. <http://quest.mda.org/files/pdfs/Part_1-newDMD.pdf>. Bushby, Katharine, Richard Finkel, and David Birnkrant. "Diagnosis and Management of Duchenne Muscular Dystrophy, Part 2: implementation of multidisciplinary care." 30 Nov. 2009. Web. 1 Dec. 2009. <http://http://quest.mda.org/files/pdfs/Part_2-newDMD.pdf>. Ciafaloni, MD, Emma, and Richard T. Moxley, MD. "Treatment Options for Duchenne Muscular Dystrophy." Current Treatment Options in Neurology 10.2 (2008): 86-93. Print. Milestones in Duchenne's Muscular Dystrophy Research. MDA.org, Feb. 2009. Web. 1 Dec. 2009. <http://www.mda.org/publications/milestones/dmd.html>. Palmieri, B., V. Sblendorio, A. Ferrari, and A. Pietrobelli. "Duchenne Muscle Activity Evaluation and Muscle Function Preservation." Obesity Reviews 9 (2008): 121-39. Print. Sayers, Stephen P. "The Role of Exercise as a Therapy for Children with Duchenne Muscular Dystrophy." Pediatric Exercise Science 12 (2000): 23-33. Print.