Download
1 / 28
280 likes | 463 Views
Infant and Young Child Feeding Policy and Strategy September 2009. Ministry of Health Royal Government of Bhutan Dr Arun Gupta MD FIAP(India). Overview. Scientific evidence in brief Status of IYCF in Bhutan Problems and underlying factors Seven strategies and action recommendations

E N D
Infant and Young Child Feeding Policy and Strategy September 2009 Ministry of Health Royal Government of Bhutan Dr Arun Gupta MD FIAP(India)
Overview • Scientific evidence in brief • Status of IYCF in Bhutan • Problems and underlying factors • Seven strategies and action recommendations • Way Forward
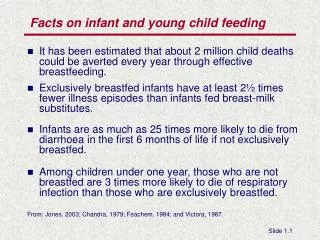
Impact of breastfeeding on Long-term health and Intelligence • Subjects who were breastfed experienced lower mean blood pressure and total cholesterol. • Prevalence of overweight/obesity was 22% higher in formula fed. • Type-2 diabetes was higher among non-breastfed subjects. • Breastfed babies had higher performance in intelligence tests. This 2007 WHO meta-analysis showed that magnitude of effect was similar to public health interventions given later.
Relative risk of suboptimum breastfeeding during first six months
Effect of nutrition-related interventions on infant mortality and DALYs (in 36 countries) Source: Zulfiqar A Bhutta et al. Maternal and Child Undernutrition Series - 3: What works? Interventions for maternal and child undernutrition and survival. January 17, 2008. www.lancet.com
Impact of Non Exclusive Breastfeeding During First Six months Due to Non- EBF 1.4 million deaths due to suboptimum breastfeeding Due to Non- EBF 43.5 million DALYs due to suboptimum breastfeeding
Effect of nutrition-related interventions on stunting (in 36 countries)
Child Survival and Nutrition Status • NMR: Not available • IMR: 40 per thousand (2007 ) • U5MR: 62 per thousand (2007) • Stunting U5 37% • Underweight 11.1% • Wasting 4.6% • LBW (2500gm or low) 9.3%
State of IYCF in Bhutan Policy and Programmes: 2008 Assessment revealed Gaps in policy and programmes ( Health system, outreach, Maternity entitlements, Code implementation and M&E etc. Practices • Good early breastfeeding within an hour : 80% • Very low exclusive breastfeeding 37% at 4 months and 10% at six months • Complementary feeding 23%
Problem Areas in IYCF • Pre- lacteal feeding. • Exclusive breastfeeding for the first six months is very rare in all, whether rural or urban communities. • Not enough milk perception is almost universal : lack of comprehensive approach. • Inadequate skills with health workers. • Breast problems like sore or cracked nipples, common but poorly managed
Problem Areas in IYCF • Use of infant formula is very high in 0-6 months being 14%. • Use of complementary food below six months is very common, rice and ‘Cerelac’ being very common. • People believe ‘Cerelac’ is a good food and want to use this even below six months in spite of the health advice. • Concept of complementary feeding after six months is not fully clear. • Policy on exclusive breastfeeding is not uniformly known • Maternity benefits are not adequate • Support level to ALL women is very low.
Underlying Factors • Cultural beliefs • Commercial promotion of baby foods • Almost all mothers perceive that their milk is not enough for the baby. • Lack of awareness about physiology of process of breastfeeding • Health workers don’t fully understand the complex hormonal control of breastfeeding. • Maternity benefits : leave of only 3 months for government workers is inadequate. • Women in un- organized sector like laborers have to return to work because of economic compulsions and not compensated for wage loss , no provision of maternity benefits for them.
3 Critical Areas • Strengthening IYCF in the Health Systems as part of standards of care • Protecting Mothers and Children below 2 years from aggressive commercial promotion of baby foods • Supporting ALL women to combine breastfeeding with work
Seven Strategic Actions • PROTECTION • PROMOTION • SUPPORT • INFORMATION(DATA BASE) • EDUCATION and TRAINING • RESEARCH • COORDINATION
Recommendations for Action Seven Strategies
Protection • Constitute a drafting committee/group to move towards legislation to protect breastfeeding from commercial influence. • Provide information about commercial sector influence to health workers on a regular basis. • Develop and implement communication campaign on complementary feeding after six months with use of local home made foods and discourage use of commercial products.
Promotion • Launch the campaigns on exclusive breastfeeding for six months. • Target teenage persons as a strategy • High level advocacy to raise the consciousness of national leaders, including the Royal Family • Expand the celebration of World Breastfeeding Week (WBW), to BHUs • Develop a plan to eliminate erroneous or incomplete information (Like e.g. belief that Cerelac or rice should be given during first six months of life). • Develop IEC materials • Campaign for economic benefits of breastfeeding
Support • Provide maternity benefits for all women, in the formal employment or unorganized sector. • Formal Sector: Increase Maternity leave, Crèches, flexi hours, work at home, expression of breastmilk facilities etc. • Create a Maternity benefit Fund for poor women in the informal sector in the rural area who have to go out to work for livelihoods. • DoR should provide paid maternity leave of six months to its women workers • Establish IYCF Counselling Centers/lactation clinics • Link exclusive breastfeeding to growth monitoring. • Revive BFHI and develop a Baby Friendly Community Imitative (BFCI) to reach to families through BHUs and ORCs.
Research • Establish a task force to conduct Infant and Young Child Feeding research. • Conduct an assessment of policy and programmes of IYCF every three years to see the trends. WBTi could be used as a tool. • In depth qualitative research on exclusive breastfeeding , use of Cerelac, rice or and other infant formula and foods very early in life, and complementary feeding. • Study impact of current HIV and infant feeding policy • Study the impact of maternity benefits on exclusive breastfeeding in one district. • Areas of research should include: • operational research on what works; • impact of breastfeeding on contraception, emotional development, obesity, • Role of skilled health counseling on exclusive breastfeeding
Information management: data base • Include early breastfeeding within one hour, exclusive breastfeeding from 0-6 months or at 6 months , and complementary feeding during 7th month in the HMIS. • Monitor exclusive breastfeeding 0-6 months at high level, at the Ministerial level, among the indicators of stunting, underweight, wasting, infant mortality and under- five mortality. • Monitor exclusive breastfeeding along with growth monitoring
Education & Training • Include concepts of optimal IYCF for health and development in curricula of primary and secondary schools, universities and community educational centers. • Strengthen IYCF in Nurses and health workers curriculum • Identify National /Regional Center/District focal points for training, education and resources and build their capacity to take this strategy forward • Develop a plan for training of all nursing staff in maternity services , the MCH staff, HAs, BHWs, to universalize reach to all people
Coordination • Establish a national IYCF committee with all sectors and having 50% women representation. • Strengthen the nutrition department at national level • Establish nutrition coordination at the regional and district centers. • Establish a budget line for IYCF in the overall health and development plans
Policy Recommendations 1. Exclusive breastfeeding • Update the existing policy to make it exclusive breastfeeding for the first six months. • Declare that infant feeding counseling is a recognized “service”in health care system. • Include exclusive breastfeeding as integral part of the HMIS. • Add a budget line for IYCF under the child nutrition and health. • Review and update policy on HIV and Breastfeeding in light of new WHO guidelines
Policy Recommendations 2. Take legislative action on protection of breastfeeding to create a long term sustainable protection
Policy Recommendations 3. Create a support system for women to combine work with breastfeeding • Extend maternity leave to 6 months, Crèches, flexi hours, making it a Legislative Action. • Create a ‘maternity benefit fund’ for helping the the poor unorganized sector women who have to resort to work for livelihoods.
Way forward • MoH should endorse and communicate widely, the policy decisions. • Create a Core group to develop an operational plan (5 years) within six months. • Plan should have clear objectives, activities, results and indicators of measurement and budgetary resources • Evaluate the plan after 3-5 years. • Plan for High level advocacy to achieve policy and programme inputs. • Begin action on capacity building within health systems.