Download
1 / 24
240 likes | 412 Views
Postoperative Adjuvant Chemotherapy (CTX) Use In Stage II/III Rectal Cancer Patients (Pts) Treated With Neoadjuvant Therapy: A National Comprehensive Cancer Network (NCCN) Analysis.

E N D
Postoperative Adjuvant Chemotherapy (CTX) Use In Stage II/III Rectal Cancer Patients (Pts) Treated With Neoadjuvant Therapy: A National Comprehensive Cancer Network (NCCN) Analysis P. Khrizman1, J. C. Niland2, A. ter Veer2, D. Milne3, K. Bullard Dunn4, W. E Carson III5, P.F. Engstrom6, S. Shibata2, J. M. Skibber7, M. R. Weiser8, D. Schrag3, A.B. Benson III1 1Robert H. Lurie Comprehensive Cancer Center of Northwestern University, Chicago, IL 2City of Hope Comprehensive Cancer Center, Los Angeles, CA 3Dana-Farber Cancer Institute, Boston, MA 4Roswell Park Cancer Institute, Buffalo, NY 5The Ohio State University Comprehensive Cancer Center - James Cancer Hospital and Solove Research Institute, Columbus, OH 6Fox Chase Cancer Center, Philadelphia, PA 7The University of Texas MD Anderson Cancer Center, Houston, TX 8Memorial Sloan-Kettering Cancer Center, New York, NY
Abstract • Background: Practice guidelines recommend that patients who receive neoadjuvant chemotherapy and radiation (nCRT) for locally advanced rectal cancer complete postoperative systemic chemotherapy irrespective of tumor downstaging. • Methods: We used the NCCN Colorectal Cancer (CRC) Database which tracks longitudinal care for patients treated at 8 specialty cancer centers* to evaluate how frequently rectal cancer patients treated with nCRT receive postoperative systemic chemotherapy. We examined patient and tumor characteristics associated with adjuvant chemotherapy (aCTX) in a multivariable logistic regression model. • Results: Between September 2005 and February 2010, 1,441 pts with stage II/III rectal cancer were enrolled. Of these, 810 pts received nCRT and were included in the analysis. Of these, 159 pts (20%) did not receive any aCTX. For those seen by a medical oncologist, the most frequent reason chemotherapy was not recommended was due to co-morbid illness (54%) and the most frequent reason chemotherapy was not received even though it was recommended or discussed was due to patient refusal (73%). Pts who were more likely to have no aCTX administered included: age 75+ (OR=11.4, p<0.0001), ECOG PS ≥ 1 (OR=3.1, p=0.0009), on Medicaid or indigent (OR=3.6, p=0.02), complete pathologic response (cPR; OR=2.4, p=0.02), abnormal CEA post-operatively (OR=2.2, p<0.0001), unavailable CEA post operatively (OR=3.4, p<0.0001), presence of re-operation/wound infection (OR=2.7, p=0.03), and no closure of ileostomy/colostomy (OR=1.9, p=0.01). • Conclusion: Even at specialty cancer centers, a sizeable minority of rectal cancer patients treated with curative intent nCR do not complete postoperative chemotherapy. Strategies to foster adherence to the third and final component of curative intent treatment are necessary. 8 specialty cancer centers include: City of Hope Cancer Center (CHCC), Dana-Farber Cancer Center (DFCC), Fox Chase Cancer Center (FCCC), Memorial Sloan-Kettering Cancer Center (MSKCC), Arthur G. James Cancer Hospital and Richard J. Solove Research Institute at the Ohio State University (OSU), Robert H. Lurie Cancer Center at Northwestern University (Lurie), Roswell Park Cancer Institute (RPCI), and University of Texas MD Anderson Cancer Center (MDA)
Introduction • In 2009 there were an estimated 40,870 new cases of rectal cancer diagnosed in the United States. • Treatment strategies for stage II/III rectal cancer patients have evolved over the past two decades to include neoadjuvant chemoradiation (nCRT) followed by surgery and post-operative adjuvant chemotherapy (aCTX). • Combinations of such treatment modalities have been shown to prolong the overall survival (OS) as well as decrease the local recurrence rates.
Introduction • NCCN Colorectal Cancer Outcomes Database Project was initiated in 2005 • Goal: evaluate the outcomes of cancer care, practice patterns and adherence to evidence-based guidelines • Participants: 8 of the 21 NCCN cancer centers • Recent published analysis: Using ASCO/NCCN quality measures, low mean concordance rates were demonstrated among participating NCCN centers for aCTX in clinical stage II/III rectal cancer within 9 months of diagnosis.
Introduction • We report an analysis of various socio-demographic and clinical variables from the cohort of locally advanced, clinical stage II/III, rectal cancer patients included in the NCCN Outcomes Database as an effort to determine the significant factors that would predict the use of aCTX following standard nCRT and surgery
Patients • Eligibility criteria: • Age 18 or older • Clinical diagnosis of locally advanced rectal cancer who received or did not receive aCTX within 9 months of diagnosis • Histologies such as adenocarcinoma, mucinous, colloid, and signet ring features included • Exclusion criteria: • Single or multiple diagnoses of colon cancer • Stage I and IV rectal cancer • Recurrent disease • No follow up • Lack of clinical staging • Less than 9 months of follow-up • Lack of documentation of administration of neoadjuvant therapy and/or surgery
Methods • Baseline patient information in the NCCN database: • socio-demographic characteristics • insurance status • co-morbidities (using Charlson index) • ECOG performance status (PS) • household income. • Medical records were systematically reviewed at 4, 8, 12 months, and then yearly to document treatment and recurrence information
Methods • 4-month assessment documentation: • clinical and pathologic TNM staging • histology • tumor location • distance from the anal verge • # of lymph nodes examined and involved with tumor • grade at diagnosis and primary surgery • presence/absence of lymphovascular invasion • Presence/absence of perineural invasion • margin involvement (proximal, distal, radial) • CEA level prior to and after surgery • surgical procedures and complications
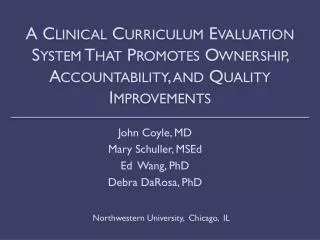
All pts with colorectal cancer N=5785 Stage II-III rectal cancer patients N=1441 Stage II-III rectal cancer patients with 9 months follow-up N=1109 Did not receive neoadjuvant therapy N=299 (27%) Did receive neoadjuvant therapy N=810 (73%) Did not receive adjuvant therapy N=159 (20%) Received adjuvant therapy N=651 (80%) Not seen by Med Onc N=21 (13%) Seen by Med Onc N=88 (55%) Unknown N=50 (31%) Chemo not recommended N=26 (30%) Chemo recommended / discussed N=52 (59%) Unknown N=10 (11%) Patients with clinical stage II/III rectal cancer and administration of adjuvant chemotherapy
Statistical Methods • The association between receipt of adjuvant therapy and each parameter was assessed independently in a univariate logistic regression model • An independent variable was created for whether the patient had been downstaged or upstaged • 52 of the patients (6%) were excluded from the downstaged/upstaged analysis (unable to stage)
Statistical Methods • Parameters found to be potentially associated with adjuvant therapy, based on a P value ≤ 0.20, were included in the initial multivariate model, along with variables known to be clinically associated with adjuvant therapy, and defined a priori • The final multivariate model includes those predictors with a 2-sided P value < 0.05 and the control variables defined a priori (clinical TNM stage and NCCN cancer center) • Point estimates of the multivariate model were reported as odds ratios (ORs) and 95% confidence intervals (CIs) for each OR
Results Reasons CTX was not recommended (26 of 88 patients) • Co-morbid illness (14 patients) • Advanced age & co-morbid illness (2 patients) • Therapy not indicated (5 patients) • Recurrence before treatment decision reached (2 patients) • Death before treatment decision reached (1 patient) • Unknown reason (2 patients)
Results Reasons CTX was recommended but was not administered (52 of 88 patients): • Declined treatment (38 patients) • Recurrence prior to treatment administration (6 patients) • Treatment not administered at 12 month assessment (2 patients) • Death before treatment administration (1 patient) • Transferred out (1 patient) • Unknown reason (4 patients)
Characteristics of N=810 clinical stage II/III rectal cancer patients who presented to NCCN institutions between September 2005 and February 2010 and received neoadjuvant therapy* F F F
Characteristics of N=810 clinical stage II/III rectal cancer patients who presented to NCCN institutions between September 2005 and February 2010 and received neoadjuvant therapy* ** *Table includes statistically significant variables only **52 of the patients (6%) were excluded from the downstaged/upstaged analyses, as these patients either had clinical TNM stage = unable to stage OR pathologic TNM stage = unable to stage
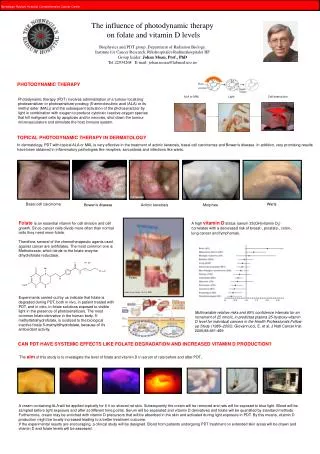
Factors associated with receiving adjuvant therapy for patients with stage II/III rectal cancer
Factors associated with receiving adjuvant therapy for patients with stage II/III rectal cancer
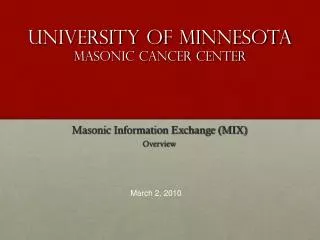
Proportion of patients in cohort that were complete responders, downstaged, upstaged, or had no change in staging * 257 of the Stage III patients (49%) were downstaged (117 pts from Stage III to II and 140 pts from Stage III to I) ** 52 of the patients (6%) were excluded from the downstaged/upstaged analyses, as these patients either had clinical TNM stage=unable to stage OR pathologic TNM stage=unable to stage
Summary • 20% of patient cohort did not receive aCTX • For patients seen by a medical oncologist, the most frequent reason aCTX was not recommended was due to co-morbid illness (54%) • For patients seen by a medical oncologist, the most frequent reason aCTX was not received although it was recommended or discussed was due to patient refusal (73%)
Summary In a multivariable model, significant factors associated with decreased administration of aCTX included: • Age >75 (OR, 0.09; 95% confidence interval (CI), 0.03-0.26, p<0.0001) • ECOG PS > 1 (OR, 0.33; 95% CI, 0.18-0.61, p=0.0009) • Abnormal/unknown CEA value after surgery (OR, 0.46; 95% CI, 0.23-0.92, p<0.0001) • Patients on Medicaid or indigent (OR, 0.28; 95% CI, 0.13-0.61, p=0.02) • Center of treatment (OR, 0.43; 95% CI, 0.21, 0.87, p=0.05) • Patients with clinical to pathologic complete response (OR, 0.42; 95% CI, 0.22-0.79, p=0.02) • Re-operation and/or wound infection (OR, 0.37; 95% CI, 0.16-0.90, p=0.03) • Lack of closure of ileostomy/colostomy (OR, 0.54; 95% CI, 0.33-0.87, p=0.01)
Discussion • The reasons patients inconsistently receive aCTX for locally advanced rectal cancer include: • Reluctance to recommend aCTX to patients with co-morbidities • Patients’ lack of acceptance of the necessary 6-month treatment • The reason for patient refusal is not recorded in NCCN database • Benefit of aCTX in locally advanced rectal cancer is not definitive and may be a reason for variability among NCCN institutions • No conclusive evidence to define the optimal aCTX regimen or the optimal subgroups of patients to treat, which can result in variability in physician recommendations
Discussion • The focus on tumor biology and patient selection generates additional data to foster adherence to aCTX guidelines
References • Jamal A, Siegel R, Ward E et al. Cancer statistics. Ca Cancer J Clin. 2009; 59: 225-249 • http://www.nccn.org/professionals/physician_gls/PDF/rectal.pdf Accessed September 2010 • Improved survival with preoperative radiotherapy in resectable rectal cancer. Swedish Rectal Cancer Trial. N Engl J Med. 1997; 336: 980-987 • Heald RJ, Moran BJ, Ryall RD, et al. Rectal cancer: the Basingstoke experience of total mesorectal excision, 1978-1997. Arch Surg. 1998; 133: 894-899 • Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery-the clue to pelvic recurrence? Br J Surg. 1982; 69: 613-616 • Kapiteijin E, Marijnen CA, Nagtegaal ID, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med. 2001; 345: 638-646 • Enker WE, Thaler HT, Cranor ML, et al. Total mesorectal excision in the operative treatment of carcinoma of the rectum. J Am Coll Surg. 1995; 181: 335-346 • MacFarlane JK, Ryall RD, Heald RJ. Mesorectal excision for rectal cancer. Lancet. 1993; 341: 457-460 • Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004; 351: 1731-1740 • Gerard JP, Conroy T, Bonnetain F, et al. Preoperative radiotherapy with or without concurrent fluorouracil and leucovorin in T3-4 rectal cancers: results of FFCD 9203. J Clin Oncol. 2006; 24: 4620-4625 • Bosset JF, Collette L, Calais G, et al. Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med. 2006; 355: 1114-1123 • Roh MS, Colangelo LH, O'Connell MJ, et al. Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: NSABP R-03. J Clin Oncol. 2009; 27: 5124-5130 • Chan AK, Wong AO, Langevin J, et al. Preoperative chemotherapy and pelvic radiation for tethered or fixed rectal cancer: a phase II dose-escalation study. Int J Radiat Oncol Biol Phys. 2000; 48: 842-856 • Das P, Skibber JM, Rodriguez-Bigas MA, et al. Clinical and pathologic predictors of locoregional recurrence, distant metastasis, and overall survival in patients treated with chemoradiation and mesorectal excision for rectal cancer. Am J Clin Oncol. 2006; 29: 219-224 • Collette L, Bosset JF, den Dulk M, et al. Patients with curative resection of cT3-4 rectal cancer after preoperative radiotherapy or radiochemotherapy: does anybody benefit from adjuvant fluorouracil-based chemotherapy? A trial of the EORTC Group. J Clin Oncol. 2007; 25: 4379-4386 • Janjan NA, Crane C, Feig BW, et al. Improved overall survival among responders to preoperative chemoradiation for localy advanced rectal cancer. Am J Clin Oncol. 2001; 24: 107-112 • Romanus D, Weiser MR, Skibber JM et al. Concordance with NCCN colorectal cancer guidelines and ASCO/NCCN quality measures: an NCCN institutional analysis. J Natl Compr Canc Netw. 2009; 7(8): 895-904 • Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chronic Dis. 1987; 40(5):P 373-383 • Vergo M, Nimeiri H, Benson AB III. Adjuvant chemotherapy after neoadjuvant chemoradiation and surgery: a quest to improve survival for stage II and III rectal cancer. Curr Colorectal Cancer Reports. 2009; 5(3): 151-157