Download
1 / 32
330 likes | 530 Views
Cost effectiveness Analysis of Non-Invasive Tools for Diagnosis of Liver Fibrosis. Abdelhamid Serwah Professor of Internal Medicine, Gastroenterology 2014. Economics is about …. Limited resources Unlimited “wants” Choosing between which ‘wants’ we can ‘afford’ given our resource ‘budget’.

E N D
Cost effectiveness Analysis of Non-Invasive Tools for Diagnosis of Liver Fibrosis Abdelhamid Serwah Professor of Internal Medicine, Gastroenterology 2014 APASL 2014, Cairo, Egypt
Economics is about … • Limited resources • Unlimited “wants” • Choosing between which ‘wants’ we can ‘afford’ given our resource ‘budget’
Economics is about choice Good ‘A’ Good ‘B’ Budget APASL 2014, Cairo, Egypt
Provision of Health Care Health Economics Provides the Tools and analytical Framework to Help Address These Objectives APASL 2014, Cairo, Egypt
‘Drummond’ checklist • Was a well-defined question posed in answerable form? • Was a comprehensive description of alternatives given? • Was there evidence that effectiveness had been established? • Were all the important and relevant costs and consequences for each alternative identified? • Were costs and consequences measured accurately/appropriately?
‘Drummond’ checklist (Cont.) 6. Were costs and consequences valued credibly? 7. Were costs and consequences adjusted for differential timing? 8. Was an incremental analysis performed? 9. Was allowance made for uncertainty? 10. Did presentation/discussion of results include all issues of concern? APASL 2014, Cairo, Egypt
Measurement: Health Outcomes • Measure effectiveness not efficacy • Efficacy = measure of effect under ideal conditions (can it work?) • Effectiveness = effect under ‘real life’ conditions (does it work?) • Efficacy does not imply effectiveness • Measure final not intermediate outcomes • Intermediate outcomes: No. Diagnosed • Final outcomes reflect change in health status • Number of lives/life years/ QUALY Gained APASL 2014, Cairo, Egypt
Sources of Effectiveness DataThe Evidence Pyramid Allows for singular insufficient data to be combined - ‘Heterogeneity’ in observations (apples and pears?) - Potential biases in searching and reviewing Bias & confounding Factors
Incremental Cost Effectiveness Ratio • ICEA= Extra Cost/ Extra benefit = (Cost 1 - Cost 2) Effectiveness 1- Effectiveness 2 APASL 2014, Cairo, Egypt
Quality-adjusted life years (QALYs) • Adjust quantity of life years saved to reflect a valuation of the quality of life • If healthy QALY = 1 • If unhealthy QALY < 1 (0.6 – 0.8 – etc) The aim is not adding years to life, but to add life to years APASL 2014, Cairo, Egypt
QALY procedure • Identify possible health states - cover all important/relevant dimensions of QoL • Derive utility ‘weights’ for each state • Multiply life years (spent in each state) by ‘weight’ for that state. APASL 2014, Cairo, Egypt
Calculating QALYs Example • Weights: • Good health = 1 • Moderate health = 0.8 • poor health = 0.5 • LYs: Year 1 + year 2 + year 3 = 3LYs (1+1+1) • QALYs: • Year 1(x0.5), year 2 (x0.8), year 3 (x1) = 2.3 QALYs (0.5+0.8+1) • Intervention may increase recovery such that • year 1(x0.8), year 2(x1), year 3(x1) = 2.8 QALYs (0.8+1+1) • No difference in LYs but gain in QALYs
Results of our Systematic Review APASL 2014, Cairo, Egypt
Cost Effectiveness of Non-invasive Methods of Diagnosis Of Liver Fibrosis In Patients With Chronic HepatitisC The aim of this review is to evaluate the evidence regarding the accuracy and Cost effectiveness of non-invasive methods and their cost effectiveness compared with liver biopsy in the diagnosis of liver fibrosis in patients with chronic hepatitis C viral infection. APASL 2014, Cairo, Egypt
Comparative Programs • Liver biopsy • Non invasive methods: • Non-invasive Tests • Elastography APASL 2014, Cairo, Egypt
Methods (PIC0) APASL 2014, Cairo, Egypt
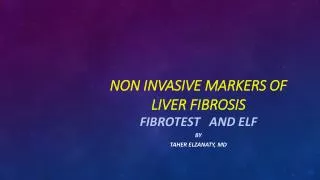
Literature Search findings • 217 citations. • 188 citations were excluded, upon screening titles and abstracts • 29 potentially relevant articles were retrieved for full-text review. • 12 potentially relevant reports retrieved from other sources (hand search, etc) • 25/41 did not meet the inclusion criteria. • 16 studies were included in this review. • Among the 16 included studies: • 4 /16 were systematic reviews • 12 were observational studies.
Selection of Included Studies 217 citations identified from electronic literature search 188 citations excluded 29 potentially relevant articles + 12 potentially relevant reports retrieved from other sources (hand search, etc) 41 potentially relevant reports 25 reports excluded: - 16 reports included in review
References • An Evaluation of the Potential Cost-Effectiveness of NoninvasiveTesting Strategies in the Diagnosis of Significant Liver FibrosisCarlson et al. 2009 • Liu S, Schwarzinger M, Carrat F, Goldhaber-Fiebert JD. Cost effectiveness of fibrosis assessment prior to treatment for chronic hepatitis C patients. PLoS ONE [Internet]. 2011 [cited 2012 Jan 19];6(12):e26783. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3229483/pdf/pone.0026783.pdf • Drummond MF, Jefferson TO, BMJ Economic Evaluation Working Party. Guidelines for authors and peer reviewers of economic submissions to the BMJ. BMJ. 1996 Aug 3;313(7052):275-83. • Drummond MF, Richardson WS, O'Brien BJ, Levine M, Heyland D. Users' guides to the medical literature. XIII. How to use an article on economic analysis of clinical practice. A. Are the results of the study valid? Evidence-Based Medicine Working Group. JAMA. 1997 May 21;277(19):1552-7. • Shaheen AA, Wan AF, Myers RP. FibroTest and FibroScan for the prediction of hepatitis C-related fibrosis: a systematic review of diagnostic test accuracy. Am J Gastroenterol. 2007 Nov;102(11):2589-600. • Halfon P, Munteanu M, Poynard T. FibroTest-ActiTest as a non-invasive marker of liver fibrosis. GastroenterolClin Biol. 2008 Sep;32(6 Suppl 1):22-39. APASL 2014, Cairo, Egypt
References • Lin ZH, Xin YN, Dong QJ, Wang Q, Jiang XJ, Zhan SH, et al. Performance of the aspartateaminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: an updated meta-analysis. Hepatol. 2011 Mar;53(3):726-36. • Shaheen AA, Myers RP. Diagnostic accuracy of the aspartateaminotransferase-to-platelet ratio index for the prediction of hepatitis C-related fibrosis: a systematic review. Hepatol. 2007 Sep;46(3):912-21. • Liu S, Schwarzinger M, Carrat F, Goldhaber-Fiebert JD. Cost effectiveness of fibrosis assessment prior to treatment for chronic hepatitis C patients. PLoS ONE [Internet]. 2011 [cited 2012 Jan 19];6(12):e26783. Available from:http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3229483/pdf/pone.0026783.pdf • Smith JO, Sterling RK. Systematic review: non-invasive methods of fibrosis analysis in chronic hepatitis C. Aliment PharmacolTher. 2009 Sep 15;30(6):557-76. • Rapid response report. Diagnosis and Monitoring of Liver Fibrosis in Patients with Chronic Hepatitis C: A Review of the Clinical Evidence and Cost Effectiveness Canadian agency for drugs and techniques in health, 2012 APASL 2014, Cairo, Egypt
Limitations of the Reviewed Studies APASL 2014, Cairo, Egypt
Limitations of the Reviewed Studies Problems with the reviewed studies: • The quality of the methods of some of the included studies was rated as poor or uncertain • Some researches were not comprehensive. • Quality assessment results for included studies were not reported. • The time interval between LB and these methods was not clearly reported or long. • In some studies patients were selected retrospectively APASL 2014, Cairo, Egypt
Limitations of the Reviewed Studies • LB has important shortcomings. • Differences in the performance of liver biopsy may therefore result in variability in the measured diagnostic accuracy of non-invasive tests across studies. • The outcomes in economic studies are varied (not unified) (cost/case detected, cost/ QALYS gained). • Some of these outcomes are not final ones. APASL 2014, Cairo, Egypt
Conclusions and recommendations APASL 2014, Cairo, Egypt
1. LB is currently the gold standard and bench mark for grading liver fibrosis in patients with CHCV. [A1] 2. LB may be associated with a small risk of serious complications. [A1] and its accuracy of LB may be compromised by many factors. [A1[ 3. The available evidence showed that the diagnostic validity of non-invasive methods for detecting liver fibrosis varied widely with the different cut-off values applied. [A2] 4. Moderate to high AUROC values up to 1.0) were reported for three tests (FT, TE, and APRI) . [A1] 5. FT was deemed to be of sufficient accuracy to replace liver biopsy in most systematic reviews. [A1]
6. Some of the systematic reviews concluded that TE and FT were less so for earlier stages of fibrosis. [B1] 7. There was generally less evidence available to recommend other tests. [B1] 9. The data to recommend that use of Non Invasive Tools in diagnostic strategies for patients with CHV is cost-effective need to be coolidated. [A2] 10. To avoid an unnecessary liver biopsy, it is reasonable to use one or multiple serum tests of fibrosis. Then liver biopsy is indicated If results of serum tests are inconclusive, or if confirmation is needed. [B1] APASL 2014, Cairo, Egypt
11. Non invasive tools will begin to replace LB. Thus, these tools are getting close to prime time. [B1] 12. Multi center researches with the following considerations are recommended using few selected tests with Standardized accuracy and cut-off points and economic studies encompassing final outcomes (QALYS), and more clinical outcomes (complications..) [A2] 13. In our circumstances, resources are scarce, and the wants are unlimited !. So, more economic studies are badly needed to provide policy makers with the best economically efficient option to offer the best care to our patients. [B1]