Download
1 / 40
420 likes | 682 Views
Advanced Dementia and Nutrition. Dr Alex Brown Consultant Elderly Care Director of Medicine and Emergency Care Bradford Teaching Hospitals NHS Trust. Bradford Nutrition Team. Matron Specialist Nurse Consultant Gastroenterologist Consultant Elderly Care Dietician ? SALT.

E N D
Advanced Dementia and Nutrition Dr Alex Brown Consultant Elderly Care Director of Medicine and Emergency Care Bradford Teaching Hospitals NHS Trust
Bradford Nutrition Team • Matron • Specialist Nurse • Consultant Gastroenterologist • Consultant Elderly Care • Dietician • ? SALT
EnteralNutrition (Tube feeding) • NG tubes • PEG feeding tubes • RIG feeding tubes • ParenteralNutrition • IV feeding
NG tubes • Short Term • Uncomfortable • Come out ( can use a bridle)
PEG/RIG Tube • Risks • Bleeding • Perforation • Infection
Question 1Old people often have grey hair • True • False
Question 2If I(you) had advanced dementia. Incontinent,Aphasic,Bed bound,No longer recognised family.I would want to consider PEG feeding. • Yes • No
Question 3If my dearest closest relative had advanced dementia. Incontinent----etc. I would want them to be considered for PEG feeding. • Yes • No
Alois Alzheimer • Female gradual cognitive decline • Feeding difficulties • Autopsy
2005 750,000 UK Dementia 2050 1,800,000
In USA • 34% of 186,835 NH residents with advanced dementia tube fed
Nutritional Problems 3 Stages: • Early • Middle • Late Exclude Reversible Cause
Early • 75% dementia sufferers at home • Reduced BMI compared to age related cohorts Social Services Family / Informal carers OT / Physio / GP Dietician Poverty Social Isolation Lack of Skill Planning and Preparation Co morbidities / Drugs Poor Mobility
Middle (? Institutional Care) Exclude Reversible Cause
Reduced Attention Span Sundowning Day / Night Reversal Feeding Difficulties Co morbidities / Drugs Environmental Factors Aids and Appliances Familiar Food Minimise Disturbance Flexibility Modified Diet / Supplements Middle (? Institutional Care)
Flexibility • Ward Routine • Fixed Meal times • Lack of Staff • Food Stuffs • Storage of Food
Late Exclude Reversible Cause
Late Eating is last ADL lost • Neuromuscular -lack of coordination • Pocket or spit food • Lack of Hunger
What to do? • Feed Orally • Tube Feeding • Treatment Goal • Prolong life • Comfort and quality of life in a terminal disease
Oral Feeding Prolong Life: May not meet needs: • Time consuming • Resource heavy (in USA fewer staff increase PEG) Aspiration:
Oral Feeding Comfort / QOL Carers concern: • Hunger / Thirst • Do not know capacity for hunger in dementia • Cancer literature – not a significant symptom Social Interaction-role for the carer
PEG Feeding Prolong life • No RCT – observational studies only • 54% mortality at 30 days • 90% die within 1 year • No difference mortality feeding tube or not • 19% PEGs inappropriate – NCEPOD • Aspiration no reduction with tube feeding • No evidence promoted healing of pressure sores • Tube placement complications
PEG Feeding Comfort / QOL • Non compliant patient – restraint • Pressure sores – no evidence of benefit ? Increased risk (diarrhoea) • No improvement in functional status • Tube complications – cellulitis, leakage, fall out Guaranteed route for drugs Chemical Physical
Cochrane Review 2009Enteral tube feeding for older people with advanced dementia • ‘No conclusive evidence that tube feeding is effective in terms of prolonging survival, improving quality of life, or leading to better nourishment or decreasing the risk of pressure sores. It may actually increase the risk of pneumonia and even death.’
Question 3If my dearest closest relative had advanced dementia. Incontinent----etc. I would want them to be considered for PEG feeding. • A. Yes • B. No
Question 3If my dearest closest relative had advanced dementia. Incontinent----etc. I would want them to be considered for PEG feeding. • Yes • No
Ros Levenson BMJ Volume 329 20th November 2004
Take Home Message • Exclude thereversible
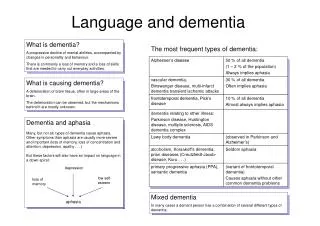
Types of Dementia Alzheimer’s Disease 55% Vascular Dementia (MID) 20% Lewy Body 15% Picks Disease 5% Other Dementia 5%
Neurofibrillary Tangles – twisted bands of fibres • Senile Plaques – dense deposits outside and around nerve cell
Summary • Dementia is a terminal disease with predictable progression – make plans • PEG unlikely to meet treatment goals • Ethics / Beliefs – prolong life ? Paramount Exclude Reversible Cause