Download
1 / 57
570 likes | 575 Views
UK Renal Registry 2012 Annual Audit Meeting. October 9 th 2012 Dr Aine Burns Consultant Nephrologist Centre for Nephrology Royal Free NHS Foundation Trust London. Conservative Kidney Management How and what can we audit?. October 9 th 2012 Dr Aine Burns Consultant Nephrologist

E N D
UK Renal Registry 2012 Annual Audit Meeting October 9th 2012 Dr Aine Burns Consultant Nephrologist Centre for Nephrology Royal Free NHS Foundation Trust London
Conservative Kidney Management How and what can we audit? October 9th 2012 Dr Aine Burns Consultant Nephrologist Centre for Nephrology Royal Free NHS Foundation Trust London
Session 5:Which decision in elderly with CKD? International Seminar on Renal Epidemiology Dr Aine Burns MD FRCP MSc Med Ed. Consultant Nephrologist, Centre for Nephrology Royal Free Hospital Campus UCL London UK Paris 22-23May 2012
Which decision in elderly with CKD? Dialysis withholding in CKD 5!"Maximum conservative management for elderly patients with renal failure stage 5"
Conservative Kidney Management: How and whatcan& should we audit? What is important to us and what is important to our patients and their close persons???
Conservative Kidney Management: How and whatcan we audit? First instance numbers Quality standards which deliver on their intent
Overview • Where we have come from • Where we are now • Where we want to go • MCM data set and Quality outcome measures
A remarkable journey! • 1964: Prof. Robin Eady and “the lucky 13!”
A remarkable journey! • 1964: Prof. Robin Eady and “the lucky 13!” • 2012: Almost 100 and going strong!
Terminology :~ • Conservative management • Maximum conservative management • Renal supportive care • Residual renal support • Conservative kidney care • The non-dialysis option • The no clearance clinic!!
A remarkable journey! • 1964: Prof. Robin Eady and “the lucky 13!” 2002-2012: MCM • 2012: Almost 100 and going strong!
Mission :D • Reverse the reversible • Preserve residual renal function • Treat inter-currant illnesses • Identify and treat symptoms • Maximize functional status • Plan end of life care • Support family and close persons • Minimize futile interventions
Not easy :?? Frailty Dementia Cognition Depression Loneliness Bereavement Mobility Functional status Advance directives Capacity Co-morbidity Inter-currant illness Falls Difficult conversations Ceilings of care Family wishes Absent relatives Hospital visits Shared care Cost
Decision aids Trade offs Health literacy
Not easy :?? Frailty Dementia Cognition Depression Lonleiness Bereavement Mobility Functional status Advance directives Capacity Co-morbidity Inter-currant illness Falls Difficult conversations Ceilings of care Family wishes Absent relatives Hospital visits Shared care Cost
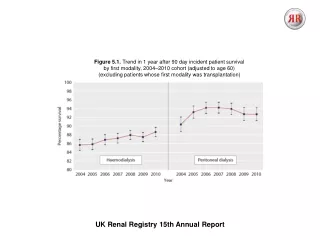
Age and Survival 1.0 < 50 Years n = 67 .9 .8 .7 50 - 65 65 -75 n = 77 n = 98 .6 P < 0.0001 Cum Survival .5 P = 0.0007 .4 > 75 Years .3 n = 48 .2 .1 0.0 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 Months on Dialysis
Survival: Carson & Burns, CJASN 2008
Survival: The MCM group were on average 6 years older than the dialysis group. Co-morbidity identical (Charlston = 7.2) Carson & Burns, CJASN 2008
Survival: Hospital free days Carson & Burns, CJASN 2008
Symptom burden Dinneen & Burns, British Renal Association Abstract 2011
Performance status End-Stage Renal Disease: A New Trajectory of Functional Decline in the Last Year of Life Fliss E.M. Murtagh PhD, Julia M. Addington-Hall PhD, Irene J. Higginson PhD. Journal of the American Geriatrics Society Volume 59, Issue 2, pages 304–308, February 2011
Patients were willing to forgo 7 months of life expectancy to reduce the number of required visits to hospital and 15 months of life expectancy to increase their ability to travel. Interpretation: Patients approaching end-stage kidney disease are willing to trade considerable life expectancy to reduce the burden and restrictions imposed by dialysis.
Treatment preferences (dialysis v. conservative care) of 105 patients with end-stage chronic kidney disease. Morton R L et al. CMAJ 2012;184:E277-E283
Quality of death: MCM patients were 4 times more likely to die at home or in a hospice Final illness short 3-7 days eGFR ± 4ml/min Pulmonary oedema rarely an issue Carson & Burns, CJASN 2008
MCM: A new phase in a remarkable journey • Legitimate & positive treatment option chosen by approx 10% of our elderly patients which delivers: • maintained functional status for many months • a short final illness • 4 times greater chance of dying at home or in hospice setting • intervention free out of hospital days may not differ much from patients who choose dialysis
Will home assisted PD influence numbers choosing MCM?? • What about un-captured patients?
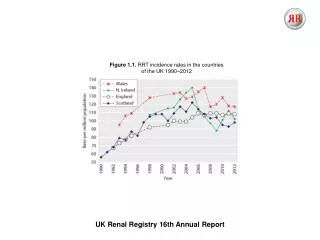
Key results During the period 2003–2007, there were nearly 21,500 new cases of ESKD in Australia, amounting to about 21 cases per 100,000 people. For every new case who receives dialysis or transplant, there is about one new case that does not.
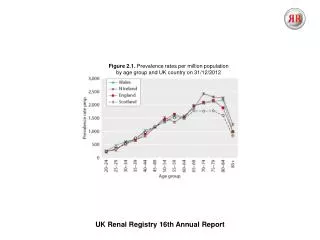
Renal Modality Age Analysis: LCC = eGFR<30 diabetic, <20 non-diabetic
Renal Modality Age Analysis: LCC = eGFR<30 diabetic, <20 non-diabetic
Conservative Kidney Management: How and what can we audit? Demographics Co-morbidity Survival Recorded cause of death Place of death Religion Post-code /deprivation score
Symptom burden Performance status/trajectories Survival & hospital free days Quality of death Decision making
Symptom burden • Performance status/trajectories • Survival & hospital free days • Quality of death (preferred place of death) • Decision making • late changes in modality • advanced care plans/advanced directives, • will availability of home assisted PD influence patient/family choice
Decision making Shared decision making Why do patients choose MCM? How & when should we have these conversations? Do many patients change their minds? The time factor!!
Decision making Shared decision making (national shared decision making programme) Why do patients choose MCM? (don’t want to be a burden/ don’t want change/ all religions & ethnic groups more or less equally represented) How and when should we have these conversations? (? as early as possible) Do many patients change their minds? (not many) The time factor!! Value of trained nurse specialists
New method for estimating the total incidence of ESKD The number of non-KRT-treated cases is estimated using a defined set of cause of death codes in the national mortality data, with the aim of counting people who died with ESKD in the study period. This number can then be added to the already available number of dialysis and transplant cases recorded on a national register. Data linkage is used to ensure that people treated with dialysis or transplant who die during the study period are only counted once.