Download
1 / 1
10 likes | 166 Views
EFFICACY OF GLYCERYL TRINITRATE (GTN) TRANSDERMAL PATCH FOR INHIBITION OF PRETERM LABOUR. Kellogg A, Kaur V, Chaudhary SC . Obstetrics & Gynaecology Department,Christian Medical College& Hospital, Ludhiana, Punjab,India 141008. Methods. Results.

E N D
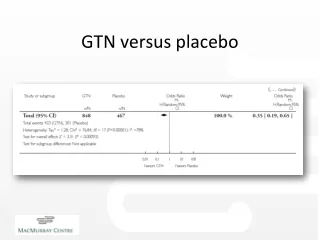
EFFICACY OF GLYCERYL TRINITRATE (GTN) TRANSDERMAL PATCH FOR INHIBITION OF PRETERM LABOUR. Kellogg A, Kaur V, Chaudhary SC. Obstetrics & Gynaecology Department,Christian Medical College& Hospital, Ludhiana, Punjab,India 141008 Methods Results • This was a prospective study conducted in department of Obstetrics and Gynaecology Christian Medical College & Hospital Ludhiana, over a period of one year. Forty-one patients were included in the study. • The mean age was 25.32 2.46 years. • The majority of patients enrolled i.e. 65.85% were primigravidae. • Women between 16 –36 weeks of gestation were included in the study. The mean period of gestation was 29 weeks 1 day 7.00. • Majority of the patients selected for the study belonged to middle income group (56.10%). 29.27% belonged to the lower income group and 14.63% of the group belonged to higher income group. • The mean number of antenatal visits was 3.66 ± 3.20. • Women with 2 or more previous abortions had a significant risk for preterm delivery. Women with no previous preterm labour had low risk for preterm delivery in our study case. • The most common antenatal complication seen was anaemia, which was present in 36.59% of the women. • The mean maternal weight of the group was found to be 64.17 ± 8.78 kgs. • There was presence of leukocytosis in 24.39% (10 patients) and this observation was statistically significant. However, positive cervical swab culture was noted in only 7.32% cases. This observation was not statistically significant. • The mean cervical effacement at the time of admission was 2.46 ± 0.69 • The mean pulse rate per minute before treatment was 85.66 ± 5.23 beats per minute. The mean pulse rate per minute after treatment was 95.00 ± 7.60 beats per minute. • The mean increase in pulse rate noted was 9.34 beats per minute after treatment with GTN transdermal Patch and this was statistically significant. • The mean drop in systolic blood pressure noted, after treatment, was 10.64 mm of Hg and this observation was statistically significant. • The mean drop in diastolic blood pressure after treatment was 7.51 mm of Hg and this observation was statistically significant. • The mean foetal heart rate, at the time of enrollment, was noted to be 143.02 ± 9.78 beats per minute. The mean foetal heart rate documented after treatment was 149.80 ± 9.57 beats per minute. • The mean increase in foetal heart rate per minute was 6.78 beats per minute and this observation was statistically significant. • The frequency of contractions ranged from 4 to 24 contractions per hour, in women who were admitted with preterm labour, at the time of enrollment. Majority of the patients (24.39%) had mild to moderate contractions Introduction Results • This study was a one-year prospective study, which was undertaken in the Department of Obstetrics and Gynaecology of Christian Medical College, Ludhiana from 1st January 2003 to 31st December 2003. • All booked and unbooked women between 20-37 weeks of gestation, coming to the department of Obstetrics and Gynaecology, with regular and painful uterine contractions (detected on cardiotocogram) associated with or without cervical changes were included in the study. • Exclusion criterion included: • Premature rupture of membranes. • Ante-partum Haemorrhage. • Hypotension indicated by a systolic pressure <90 mm Hg or a diastolic pressure < 60 mm Hg. • Chorioamnionitis • Major fetal abnormalities • Cervical suture in-situ. • History of any medical condition that would contradict the drug. • Unexplained pyrexia. • Other tocolytic therapy • A detailed obstetrical and medical history was taken to rule out condition which would contradict the usage of GTN Patch. • A general physical and systemic examination was then carried out. Vital signs were noted. Per abdomen examination was done to detect if patient was having contractions. Frequency and duration of the contractions ware noted, along with the fetal heart rate. A cardiotocogram (CTG) tracing of twenty minutes was taken to document the frequency and duration of the uterine contractions. • A sterile per speculum examination was done to rule out premature rupture of membranes, cervical swab taken and sent for culture sensitivity. A per vaginal examination was done on admission to note the cervical effacement and dilatation. Total and Differential blood cell counts were sent on admission. • Subjects with preterm labour satisfying the criteria for preterm labour were started on GTN, after taking informed consent. 10 mg of GTN patch was applied to the abdomen. If uterine contractions did not subside by 2 hours (recorded on a repeat CTG of twenty minutes), another 10mg patch was applied. Not more than two patches (20mg) were applied per 24 hours to the same patient. The patches were removed every 24 hours and a fresh patch was applied until uterine contractions subsided completely for 24 hours or for a maximum of seven days. • Enrolled cases were given supportive management of bed rest and were hydrated with 1 litre of Ringer Lactate, which was infused over a period of 2 hrs. 2 doses of 12 mg Betamethasone intramuscular injection were given 12 hourly to hasten foetal lung maturity. • Maternal pulse, blood pressure and fetal heart rate were monitored every 15 minutes for the first one-hour and subsequently every hourly. Any side effect experienced by the patient was noted down. The time of cessation of contractions and the treatment to delivery time were also noted. • Cases were followed upto delivery. The mode of delivery, Apgar Score at 1 minute and 5 minutes, birth weight were noted. Postpartum complications, if occurred, were noted..Tocolysis was considered effective if delivery was delayed beyond 48 hours • The statistical data was analyzed by using multivariate regression analysis. Preterm delivery,defined as onset of labour before completion of 37 weeks, represents one of the major unsolved problems in obstetrics and gynaecology with its associated mortality and morbidity. The incidence of preterm birth in India is 10-15% of all births whereas in developed countries it lies between 5-10% 1 Apart from the high mortality, a large percentage of the preterm neonates suffer from severe neonatal complications that occur afterwards. These complications include respiratory distress syndrome, intraventricular haemorrhage, sepsis and necrotizing enterocolitis and long term sequelae like cerebral palsy, microcephaly, blindness due to retrolental fibrosis, deafness and mental retardation. 2 Studies have shown that a small increase in the period of gestation can have an important effect on survival. 3,4 Increased attention to prevention of prematurity has become the focus of prenatal care now. Though, research into the causes, treatment and prevention of preterm labour is being carried out, these advances have not been highly effective in preventing the early delivery of the foetus. Thus, tocolysis remains the most effective way to delay premature delivery and improve neonatal outcome. Maternal and foetal side effects of most of the tocolytics available limit their clinical usefulness. Thus, there is need for an effective tocolytic with minimal side effects. Glyceryl Trinitrate (GTN), a nitric oxide donor; holds the prospect of being an efficacious tocolytic, which can be used for maintenance or prophylaxis in preterm labour. This is due to its possible effect in reducing preterm delivery with fewer maternal and foetal side effects and lower maternal discontinuation rates The current study was undertaken with an attempt to understand the efficacy of GTN transdermal patch as a potent tocolytic, in search of a better tocolytic with fewer side effects and better compliance. • 34.16% of patients achieved complete tocolysis by 2 hours of application of GTN transdermal patch. Maximum dosage used was 20mg of GTN. • The mean time of cessation of contractions, after application of GTN Patch was 4.76 ± 4.67 hours. Failure of tocolysis was noted in 4 patients (9.76%) in the study. • The mean number of days, by which delivery was postponed, was 24.33 ± 11.56 days, in women treated with GTN Patch. It was seen that 78.38% patients, in whom preterm labour was effectively inhibited, went into labour after 36 weeks of gestation. No patient delivered before 28 weeks. • Effective tocolysis (delay in delivery > 48 hours) was seen in 37 patients (90.24%) and this observation was statistically significant • 41.46% patients had normal vaginal delivery, forceps application was needed in 9.76% and 48.78% underwent caesarean section. • The mean Apgar Score at 5 minutes of birth was found out to be 8.72 ± 0.72. No case in the study had Apgar Score less than 3 at 5 minutes. • Majority of the birth weight of babies delivered by women treated with GTN were between 2000 –3000grams (65.85%). • The side effects developed were minor in nature like headache, nausea and skin rash and in no patient discontinuation of treatment was required. Conclusions It is thus concluded from this study that GTN Transdermal Patch is an efficacious tocolytic which can inhibit labour. Minor maternal side effects, no adverse effect on the foetus and higher patient compliance make it a convenient therapy to administer. References Chopra S: Preterm in labour: Use of tocolytics for prolongation of pregnancy. Obs & Gynae Today 1997; 2: 28-30. Singh M: Care of the newborn. Sagar Publications, New Delhi. 4th Edition 1991; 117-125. Rush RW, Davey DA and Segall ML: The effect of preterm delivery on perinatal mortality. Br J ObstetGynaecol 1978; 85: 806-811. Check WA: FDA considers a first: approval of tocolytics for prolongation of labour. JAMA1980; 243:1313-1314. Objectives • The study was undertaken with the aim of • Evaluating the efficacy of GTN transdermal patch for inhibition of preterm labour. • 2) Recording the adverse effects, if any, associated with the use of GTN patch as a tocolytic.