Download

1 / 22
220 likes | 230 Views
Community-Associated Methicillin-Resistant Staphylococcus aureus. Ruth Lynfield, M.D. Minnesota Department of Health. Emergence of Resistance in S. aureus. Chambers, EID 7:178-182, 2001. Methicillin Resistance in S. aureus. mec A confers resistance to penicillins and cephalosporins

E N D
Community-Associated Methicillin-Resistant Staphylococcus aureus Ruth Lynfield, M.D. Minnesota Department of Health
Emergence of Resistance in S. aureus Chambers, EID 7:178-182, 2001
Methicillin Resistance in S. aureus • mecA confers resistance to penicillins and cephalosporins • mecA is part of the staphylococcal cassette chromosome mec (SCCmec), a mobile genetic element (21-67 kb in size) that may also contain genes that confer resistance to non-beta-lactam antimicrobials • SCCmec has been classified into 5 main types based on polymorphisms in its conserved genes
HVR mecI mecR1 mecI mecR1 Staphylococcal Cassette Chromosome mec Types SCCmec type I - Archaic clone LJ RJ D mecR1 dcs orfX pls HVR IS1272 ccrAB1 SCCmec type IA - Iberian clone LJ RJ DHVR DmecR1 orfX dcs pls pUB110 IS1272 ccrAB1 SCCmec type III - Hungarian clone LJ RJ ips YccrAB orfX pT181 YTn554 pI258 Tn554 ccrAB3 SCCmec type IIIA - Brazilian clone LJ RJ YccrAB orfX pI258 YTn554 HVR Tn554 ccrAB3 SCCmec type II - NY/Japan clone 10Kb LJ RJ dcs orfX kdp Tn554 HVR pUB110 HVR mecI mecR1 mecI mecR1 ccrAB2 mecA IS431 SCCmec type IV - Pediatric clone LJ RJ LJ - chromosomal left junction RJ - chromosomal right junction dcs orfX DmecR1 HVR IS1272 ccrAB4 Oliveira et al., Lancet ID, 2002
Background: Healthcare-associated (HA) MRSA • Leading cause of nosocomial pneumonia, surgical wound infection, and bloodstream infection • Established risk factors include • Current or recent hospitalization • Residence in long-term care facilities • Dialysis • Typical resistance profile • Resistant to many antimicrobials in addition to beta-lactams
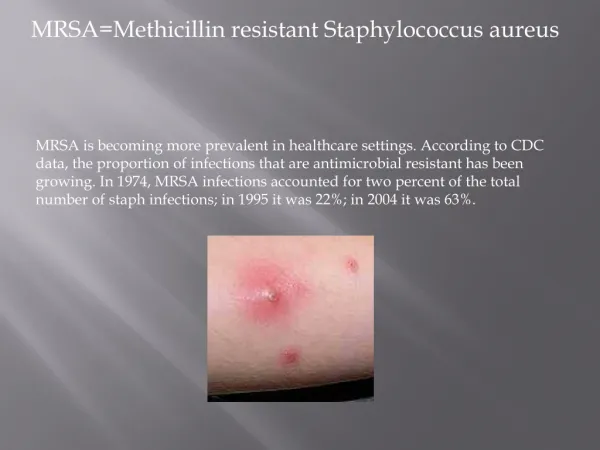
Community-Associated Methicillin-Resistant Staphylococcus aureus (CA-MRSA) Reports began in 1980s of MRSA occurring in the community in patients without established risk factors • Younger patients • Indigenous peoples and racial minorities • Skin infections common • Outbreaks: • Injection drug users • Players of close-contact sports • Prison/jail inmates • Group Homes (developmentally disabled) • Men who have sex with men
CA-MRSA • Isolates typically susceptible to most antimicrobial classes other than beta-lactams • Isolates differ by PFGE from HA-MRSA • Isolates have different SCCmec types from HA-MRSA • Isolates have been identified that are highly related to MSSA except for SCCmec element* • Although most infections associated with CA-MRSA have been skin and soft tissue, some infections have been very severe including necrotizing pneumonia and other life-threatening infections * Fey. Antimic Agents Chem. 2003; 47: 196-203. Mongkolrattanothai. Clin Infec Dis. 2003: 37: 1050-8.
CA-MRSA in Minnesota • 1997- Minnesota Department of Health (MDH) received reports of MRSA infections in young, previously healthy individuals • Reported four pediatric deaths due to MRSA infection (MMWR, August 20, 1999)
Case 1 Case 2 Case 3 Case 4 Age 7 years 16 months 13 years 12 months Gender Female Female Female Male Race African American American Indian White White Syndrome Septic joint, pneumonia/ empyema Sepsis Necrotizing pneumonia/ sepsis Necrotizing pneumonia/ sepsis Antimicrobial susceptibility T/S, tet, cip, gent, ery, clind, vanc T/S, tet, cip, gent, ery, clind, vanc T/S, tet, cip, gent, ery, clind, vanc T/S, tet, cip, gent, ery, clind, vanc PFGE Clonal group A Clonal group A (MW2) Clonal group A Clonal group A Four Pediatric Deaths, CA-MRSA Minnesota and North Dakota, 1997-99
CA-MRSA in Minnesota Minnesota Communicable Disease Reporting rule amended in 1999: • All cases of serious illness or death due to CA-MRSA reportable • Sentinel sites were required to report all cases of MRSA
Minnesota Definition of CA-MRSA Used in Prospective Surveillance • Positive culture for MRSA obtained within 48 hours of admission (if hospitalized) • No history of hospitalization in past year • No history of surgery in past year • No history of long-term care in past year • No history of dialysis in past year • No permanent indwelling catheters or percutaneous medical devices • No prior history of MRSA infection or colonization
Healthcare-associated • Hospital-acquired • Community-onset with Risk factors Minnesota MRSA Surveillance MRSA patients Risk factors (+) Medical record review Risk factors (-) Community-onset, no risk factors documented in medical record Telephone interview Indeterminate No interview Risk factors (+) Risk factors (-) Community-associated
Prospective MRSA Surveillance: Methods, MN, 2000 • 12 sentinel hospitals selected to represent different geographic regions (6 metro area, 6 greater MN) reported all cases MRSA • Patient information was collected and MRSA isolates were obtained for all cases (HA and CA-MRSA) • Presumptive CA-MRSA patients were interviewed to verify that they met the CA-MRSA case definition
Minnesota MRSA Surveillance Methods: Laboratory • MRSA isolates from sentinel sites sent to MDH Laboratory • All CA-MRSA isolates tested • 25% of HA-MRSA isolates from each site randomly selected for testing • Isolates confirmed as S. aureus (tube coagulase) • Antimicrobial susceptibility testing (including oxacillin) by broth micro-dilution • PFGE subtyping • 26 CA and 26 HA-MRSA isolates characterized for toxins
Minnesota MRSA Surveillance Results: 2000 • 4,612 patients with S. aureus identified at 10 sentinel sites in 2000 (total number S. aureus unavailable at two sites) • 1100 (25%) were MRSA (range 10-49%) • 937 (85%) were HA-MRSA • 131 (12%) were CA-MRSA (range 4-50%) after patient interview* • 32 (3%) not enough information to classify *13% of presumptive CA-MRSA cases were reclassified as HA-MRSA after interview
CA and HA-MRSA PFGE Subtype Patterns, Minnesota, 2000 Healthcare-associated (clonal group H) Community-associated (clonal group A)
PFGE Relatedness of CA and HA-MRSA Isolates to Reference Strain, MN, 2000 Relatedness to Reference Strain 100% 90% 70% 50% 35% 15% 130 120 Clonal Group A 110 Community-associated (n=106) Healthcare-associated (n=211) 100 90 80 70 Number of Isolates 60 50 40 30 20 10 0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 (MW2) Number of Bands Different from MRSA Reference Strain
Initial Empiric Treatment of CA-MRSA Infections, MN, 2000 (n = 92)
Susceptibility of CA and HA-MRSA Isolates by Antimicrobial Agent, MN, 2000 100 100 95 96 94 94 92 92 90 83 79 80 44 21 16 9 p<0.001 p<0.001 p<0.001 p=0.001
Trends in Antimicrobial Susceptibility of CA-MRSA Isolates, MN, 1996-2001 • No significant change in susceptibilities to tetracycline, TMP-SMX, gentamicin, or rifampin • Susceptibility decreased over time: • Ciprofloxacin: 92% to 77%, x2 trend=15.3, p<0.001 • Clindamycin: 90% to 80%, x2 trend=4.1, p<0.05 • Erythromycin: 70% to 39%, x2 trend=14.8, p<0.001
Efflux pump Methylase Macrolides Macrolide Resistance Mechanisms in S. aureus Macrolides (e.g., erythromycin) Lincosamides (e.g., clindamycin) Streptogramin B Protein synthesis erm msrA Ribosome Macrolides Lincosamides Streptogramin B