Download
1 / 2
20 likes | 91 Views
D EVELOPING SELF-MANAGEMENT SUPPORT FOR LONG TERM CONDITIONS – USING ETHNOGRAPHY TO TELL THE STORY

E N D
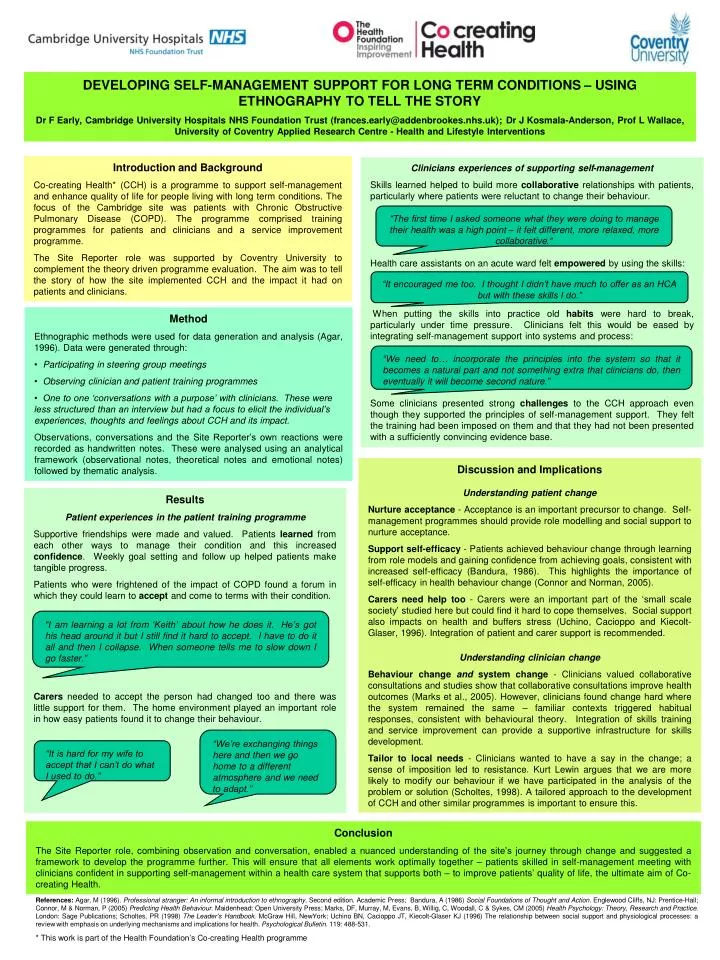
DEVELOPINGSELF-MANAGEMENT SUPPORT FOR LONG TERM CONDITIONS – USING ETHNOGRAPHY TO TELL THE STORY Dr F Early, Cambridge University Hospitals NHS Foundation Trust (frances.early@addenbrookes.nhs.uk); Dr J Kosmala-Anderson, Prof L Wallace, University of Coventry Applied Research Centre - Health and Lifestyle Interventions Introduction and Background Co-creating Health* (CCH) is a programme to support self-management and enhance quality of life for people living with long term conditions.The focus of the Cambridge site was patients with Chronic Obstructive Pulmonary Disease (COPD).The programme comprised training programmes for patients and clinicians and a service improvement programme. The Site Reporter role was supported by Coventry University to complement the theory driven programme evaluation. The aim was to tell the story of how the site implemented CCH and the impact it had on patients and clinicians. Clinicians experiences of supporting self-management Skills learned helped to build more collaborative relationships with patients, particularly where patients were reluctant to change their behaviour. Health care assistants on an acute ward felt empowered by using the skills: When putting the skills into practice old habits were hard to break, particularly under time pressure. Clinicians felt this would be eased by integrating self-management support into systems and process: Some clinicians presented strong challenges to the CCH approach even though they supported the principles of self-management support. They felt the training had been imposed on them and that they had not been presented with a sufficiently convincing evidence base. “The first time I asked someone what they were doing to manage their health was a high point – it felt different, more relaxed, more collaborative.” “It encouraged me too. I thought I didn’t have much to offer as an HCA but with these skills I do.” • Method • Ethnographic methods were used for data generation and analysis (Agar, 1996). Data were generated through: • Participating in steering group meetings • Observing clinician and patient training programmes • One to one ‘conversations with a purpose’ with clinicians. These were less structured than an interview but had a focus to elicit the individual’s experiences, thoughts and feelings about CCH and its impact. • Observations, conversations and the Site Reporter’s own reactions were recorded as handwritten notes. These were analysed using an analytical framework (observational notes, theoretical notes and emotional notes) followed by thematic analysis. “We need to… incorporate the principles into the system so that it becomes a natural part and not something extra that clinicians do, then eventually it will become second nature.” Discussion and Implications Understanding patient change Nurture acceptance - Acceptance is an important precursor to change. Self-management programmes should provide role modelling and social support to nurture acceptance. Support self-efficacy - Patients achieved behaviour change through learning from role models and gaining confidence from achieving goals, consistent with increased self-efficacy (Bandura, 1986). This highlights the importance of self-efficacy in health behaviour change (Connor and Norman, 2005). Carers need help too - Carers were an important part of the ‘small scale society’ studied here but could find it hard to cope themselves. Social support also impacts on health and buffers stress (Uchino, Cacioppo and Kiecolt-Glaser, 1996). Integration of patient and carer support is recommended. Understanding clinician change Behaviour changeandsystem change - Clinicians valued collaborative consultations and studies show that collaborative consultations improve health outcomes (Marks et al., 2005). However, clinicians found change hard where the system remained the same – familiar contexts triggered habitual responses, consistent with behavioural theory. Integration of skills training and service improvement can provide a supportive infrastructure for skills development. Tailor to local needs - Clinicians wanted to have a say in the change; a sense of imposition led to resistance. Kurt Lewin argues that we are more likely to modify our behaviour if we have participated in the analysis of the problem or solution (Scholtes, 1998). A tailored approach to the development of CCH and other similar programmes is important to ensure this. Results Patient experiences in the patient training programme Supportive friendships were made and valued.Patients learned from each other ways to manage their condition and this increased confidence.Weekly goal setting and follow up helped patients make tangible progress. Patients who were frightened of the impact of COPD found a forum in which they could learn to accept and come to terms with their condition. Carers needed to accept the person had changed too and there was little support for them. The home environment played an important role in how easy patients found it to change their behaviour. “I am learning a lot from ‘Keith’ about how he does it. He’s got his head around it but I still find it hard to accept. I have to do it all and then I collapse. When someone tells me to slow down I go faster.” “We’re exchanging things here and then we go home to a different atmosphere and we need to adapt.” “It is hard for my wife to accept that I can’t do what I used to do.” Conclusion The Site Reporter role, combining observation and conversation, enabled a nuanced understanding of the site’s journey through change and suggested a framework to develop the programme further. This will ensure that all elements work optimally together – patients skilled in self-management meeting with clinicians confident in supporting self-management within a health care system that supports both – to improve patients’ quality of life, the ultimate aim of Co-creating Health. References: Agar, M (1996). Professional stranger: An informal introduction to ethnography. Second edition. Academic Press; Bandura, A (1986) Social Foundations of Thought and Action. Englewood Cliffs, NJ: Prentice-Hall; Connor, M & Norman, P (2005) Predicting Health Behaviour. Maidenhead: Open University Press; Marks, DF, Murray, M, Evans, B, Willig, C, Woodall, C & Sykes, CM (2005) Health Psychology: Theory, Research and Practice. London: Sage Publications; Scholtes, PR (1998) The Leader’s Handbook. McGraw Hill, NewYork; Uchino BN, Cacioppo JT, Kiecolt-Glaser KJ (1996) The relationship between social support and physiological processes: a review with emphasis on underlying mechanisms and implications for health. Psychological Bulletin. 119: 488-531. * This work is part of the Health Foundation’s Co-creating Healthprogramme