Download
1 / 29
460 likes | 1.08k Views
Stress Physiology. Mind/Body Health RRCC Holistic Health Spring 2011. Stress Response. Exhaustion stage- hormones don’t get depleted The stress response becomes more damaging than the stressor- the body spends energy on stress and defense at the expense of growth, reproduction, etc.

E N D
Stress Physiology Mind/Body Health RRCC Holistic Health Spring 2011
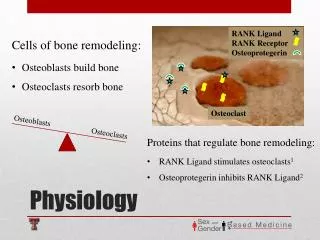
Stress Response • Exhaustion stage- hormones don’t get depleted • The stress response becomes more damaging than the stressor- the body spends energy on stress and defense at the expense of growth, reproduction, etc. • Hormones • Catecholamines- epi and norepi- act within seconds • Glucocorticoids- steroids- cortisol- minutes to hours • HPA axis- CRH (corticotropin releasing hormone) in hypothalamus, ACTH (adrenocorticotropic hormone) in anterior pituitary, glucocorticoids in adrenal • Glucagon- hungry state- mobilizes energy stores • Prolactin- suppresses reproduction • Endorphins and enkephalins- blunt pain perception • Vasopressin (ADH)- holds water in blood • Inhibited- reproductive hormones, growth hormones, insulin
Stress Response • Glucocorticoids- increase and maintain blood glucose • Gluconeogenesis in liver, amino acid mobilization, inhibition of glucose uptake, fat breakdown • Immune suppression, degradation of wbc’s • Increases blood cholesterol • Why do we need them if natural stressors are acute? • Mediate stress response, but also recovery from it • And prepare for the next one • Stress signatures- each stressor subtly different • SNS and glucocorticoids consistent • Speed and magnitude of both can vary • SNS active in subordinate rat who’s vigilant and trying to cope with a challenge, cortisol more in rat who’s given up • Not all other hormones always activated • Tissue sensitivity to hormones also changes • Psychological context
Stress and the Heart • Acute stress- HR up, BP up, arteries to mm and vital organs dilate, nonessential arteries constrict, blood flow to kidneys and kidney function down • So why do we pee our pants? • Vigilance- HR, blood flow down, vascular resistance up
Stress and the Heart • Chronic stress • Hypertension- BP up chronically • And small vessels have to work harder to regulate local blood flow, so they get more muscular, more rigid, raising BP… • Left ventricular hypertrophy- blood returns to the heart with more force, heart muscle thickens • Irregular heartbeat more likely • Greater demand for blood • LV hypertrophy- after age, the best predictor of cardiac risk • Blood vessels- damage at bifurcation points • No cell in the body is more than 5 cells away from a blood vessel, yet the circulatory system is 3% of body mass • Inflammatory response, foam cells full of fat • Epinephrine increases platelet activity • Also mobilizing fat, glucose, LDL cholesterol into bloodstream • Vessel damage a better predictor of HD than cholesterol • C-reactive protein (CRP)
Stress and the Heart • Plaques • Ischemia- impaired blood flow • Angina pectoris- heart, myocardial infarction • Claudication- lower body • Thrombus- blood moving with more force more likely to tear the plaque loose • Vast majority of MI’s and strokes • Myocardial ischemia- coronary arteries normally dilate in response to stress • But in chronic ischemia, they vasoconstrict • The damaged CV system is hypersensitive to acute physical or psychological stressors • Sudden cardiac death- extreme acute stress causing ventricular arrhythmia or fibrillation
Stress and Immunity • The immune system sorts self from nonself • Acquired immunity • Can target a specific pathogen • Takes time to build up • Now geared to go after the pathogen, and boosted with repeated exposure • Innate immunity • Saliva, mucosal surfaces • Capillary dilation at site • Macrophages, neutrophils, natural killer cells
Cellular Stressors • Hypoxia- decreased oxygen • Nutritional imbalance- ex. diabetes • Physical- temperature, radiation, mechanical trauma, electric shock • Chemical- poisons, drugs, etc. • Infectious- viruses, bacteria, fungi, protozoa, nematodes • Genetic • Psychogenic
Local Adaptation Syndrome • Cellular immune response • Designed to neutralize, control, or eliminate the offending agent • Inhibited by chronic stress
B and T Cell Formation • B cells- humoral(blood) immunity • T cells- cell-mediated immunity • Both- white blood cells or leukocytes • Both work together in immune response (along with monocytes)
B Cell Activation • B cells make antibodies; some have memory
T Cell Activation • T cells kill infected cells and secrete immune chemicals
Antibody-Mediated Immune Response • B cells secrete antibodies which bind to antigens, enabling Ab-Ag complex to be cleared • B cell antibodies bind to antigens so body can clear them- T cells secrete cytokines which help B cells to mature
Cell-Mediated Immune Response • T cells kill cells with Ag and self Ag • T cells mobilized when they encounter B cells with Ag fragments
Stress and Immunity • The immune sorting process • Dangerous seen as safe- infectious disease • Safe seen as dangerous- allergy, autoimmune disease • Multiple sclerosis, juvenile diabetes, rheumatoid arthritis, lupus, etc. • Stress • Suppresses lymphocyte (wbc) formation and release • Shortens time that wbc’s in circulation • Inhibits antibody formation • Disrupts wbc communication • Inhibits innate immunity, suppressing inflammation • Glucocorticoids most prominent, but others contribute
Stress and Immunity • Acute stress enhances immunity, particularly innate • More immune cells in circulation, more at site, better communication, more Ab’s in saliva • Glucocorticoids and SNS both involved • Cortisol (early in a stressor) kills older wbc’s, sculpting stress response, and deploys wbc’s to site of infection • But after about an hour, cortisol and SNS activation starts to dampen the immune response • Why? To bring it back down to baseline • This is part of the recovery from the stress response • Adaptive until chronic stress leads to suppression • People with autoimmune diseases (rheumatoid arthritis, for ex) have glucocorticoid suppression or less tissue sensitivity to cortisol
Autoimmunity • Overactivation of the immune system • Steroid treatment- glucocorticoids to suppress immune system • Prolonged major stressors decrease autoimmune Sx in lab rats • But stress is among the most reliable factors in worsening autoimmune diseases • Numerous transient stressors ratchet the system in the direction of autoimmunity • Massive stressors suppress immunity
Stress and Metabolism • Rapid energy mobilization • Insulin secretion down • Glucocorticoids block nutrient transport into fat cells • GC’s, glucagon, epi, norepi • TG’s broken down in fat cells- FFA’s and glycerol in blood • Glycogen broken down to glucose • Protein to amino acids • Gluconeogenesis- glucose made from the amino acids • GC’s block energy uptake into fat cells and muscles • Exercising muscles override this blockade • Good for freeing energy in acute stress and normally
Chronic Stress and Metabolism • Inefficient- it costs energy to mobilize energy • Muscle wasting- not usually a problem, but myopathy possible in steroid patients • The fat and sugar in the blood worsens CVD • And stress increases LDL and lowers HDL
Diabetes • The body’s insulin is insufficient for its needs, so blood sugar is too high • 20.8 million in US have diabetes- 7% of population • Type I- insulin-dependent • Childhood onset • Less common • Requires insulin shots • Type II- insulin-resistant • Adult (or teen) onset • More common (90-95%) • Diet and lifestyle related- obesity • Treated with diet, exercise, meds, insulin shots
Diabetes and the Pancreas • Pancreas makes digestive enzymes, and… • Islets of Langerhans in pancreas make insulin
Diabetes and the Pancreas • Insulin signals “fed state” and signals body to move glucose from blood to tissues • Underproduction or insensitivity causes blood sugar to remain high • Type I- insulin production genetically impaired • Type II- pancreas wears out and/or insulin resistance
Diabetes • Risk Factors • Western diet • Obesity- largest factor • Physical inactivity • Early Signs • Frequent urination • Excessive thirst • Craving for sweets and starches • Weakness • Complications • Heart disease • Stroke • Kidney disease • Retinopathy • Neuropathy • Foot complications • Skin complications • Gestational diabetes • 2 of 3 with diabetes die of heart disease or stroke
Obesity and Diabetes • Type 2 DM • Fat cells distend and respond less to insulin • Less glucose and fat taken up- CV damage • Hormones then trigger fat and muscle to become more insulin-resistant • Pancreas secretes more insulin • Vicious circle, leading to islet cell burnout and type I DM
Stress and Diabetes • More glucose and fat in the blood • Glucocorticoids make fat cells less sensitive to insulin • Stress promotes insulin resistance • Higher rates of major stressors in the three years before onset (of type I) • Stress can encourage the immune system to attack the pancreas • Stress increases the chances of getting DM, accelerates its development, and encourages the major complications
Stress and Eating • 2/3 hyperphagic, 1/3 hypophagic • CRH (hypothalamus, HPA axis) suppresses appetite • Glucocorticoids stimulate appetite • Preferentially for starch, sugar, fat • And blunt satiation signal of leptin from full fat cells • What’s going on? • CRH secreted and cleared faster- seconds • GC’s minutes to hours • Acute stress- high CRH, low GC- low appetite • Sustained stress- high CRH, high GC • The CRH overrides the GC- low appetite • Recovery period- low CRH, high GC- high appetite
Stress and Eating • So in acute stress, a few minutes of high CRH, hours of high GC- appetite stimulated • Chronic nonstop stress- high CRH and GC- appetite suppression • Frequent intermittent stressors • Bursts of CRH, constant GC elevation- munchies • Also, people secrete GC’s differently- amounts, and time to return to baseline • The hypersecreters are more likely hyperphagic, especially for sweets • Hyperphagia also more in emotional eaters and in normally “restrained” eaters
Apples and Pears • GC’s stimulate fat storage in presence of high insulin • High GC, low insulin = stressor • High GC, high insulin = recovery • Abdominal fat cells more sensitive • A large WHR (waist to hip ratio) is a better predictor of metabolic trouble than obesity • Fat released from abdominal fat cells goes to the liver and is converted to glucose • High blood sugar, insulin resistance • Apples, not pears, tend to have prolonged GC response • And- the comfort foods and the abdominal fat are stress-reducers
Metabolic Syndrome • AKA “Syndrome X” • Cluster of symptoms • Hyperinsulinemia • Glucose intolerance • Hyperlipidemia • Hypertension • CA not in metabolic syndrome, but patterns of incidence related • These predict each other and major disease outcomes