Download
1 / 49
590 likes | 2.3k Views
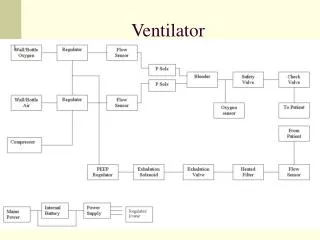
Ventilator-induced Diaphragmatic Dysfunction. Dr Bobby King Pamela Youde Nethersole Eastern Hospital, Hong Kong 23 rd December 2011. Mechanical ventilation. Origins of mechanical ventilation. The era of intensive care medicine began with positive-pressure ventilation.

E N D
Ventilator-induced Diaphragmatic Dysfunction Dr Bobby King Pamela Youde Nethersole Eastern Hospital, Hong Kong 23rd December 2011
Origins of mechanical ventilation The era of intensive care medicine began with positive-pressure ventilation • Negative-pressure ventilators (“iron lungs”) • Non-invasive ventilation first used in Boston Children’s Hospital in 1928 • Used extensively during polio outbreaks in 1940s – 1950s • Positive-pressure ventilators • Invasive ventilation first used at Massachusetts General Hospital in 1955 • Now the modern standard of mechanical ventilation The iron lung created negative pressure in abdomen as well as the chest, decreasing cardiac output. Iron lung polio ward at Rancho Los Amigos Hospital in 1953.
Indications • Respiratory Failure • Apnea / Respiratory Arrest • inadequate ventilation (acute vs. chronic) • inadequate oxygenation • chronic respiratory insufficiency
Indications • Cardiac Insufficiency • eliminate work of breathing • reduce oxygen consumption • Neurologic dysfunction • central hypoventilation/ frequent apnea • patient comatose, GCS < 8 • inability to protect airway
Complications • infection, • barotrauma, • volutrauma, • cardiovascular compromise, • tracheal injuries, • oxygen toxicity, • ventilator-induced lung injury …
Optimal ventilatory care? • Minimize complications • Facilitate weaning
Weaning from ventilator • Difficulties in discontinuing ventilatory support are encountered in 20–25% of mechanically ventilated patients • A comparison of four methods of weaning patients from mechanical ventilation. Spanish Lung Failure Collaborative Group. N Engl J Med 1995;332:345–350. • 40% of time spent in the intensive care unit being devoted to weaning • Modes of mechanical ventilation and weaning: a national survey of Spanish hospitals. Spanish Lung Failure Collaborative Group. Chest 1994;106:1188–1193. • respiratory muscles play a pivotal role in determining the weaning outcome • Respiratory muscles and weaning failure. Eur Respir J 1996;9:2383–2400.
Mechanical ventilation itself could contribute to weaning difficulties • due to atrophy and other disuse effects on the respiratory muscles
Definition of VIDD • Ventilator induced diaphragmatic dysfunction (VIDD): • a loss of diaphragmatic force-generating capacity • that is specifically related to the use of mechanical ventilation • Vassilakopoulos T, Petrof BJ. Ventilator-induced diaphragmatic dysfunction. Am J Respir Crit Care Med 2004;169(3):336–341.
Diagnosis of VIDD • A diagnosis of exclusion • history of having undergone a period of controlled mechanical ventilation (CMV), • other possible causes of diaphragmatic weakness having been sought and ruled out • Suspect VIDD if a patient who fails to wean after a period of CMV
To rule out … • Other known causes of respiratory muscle weakness such as • shock, • ongoing sepsis, • major malnutrition, • electrolyte disturbances, and • neuromuscular disorders acquired in the intensive care unit
How to exclude …? • prolonged neuromuscular blockade • excluded by the lack of an abnormal response to train-of-four stimulation • critical illness polyneuropathy • absence of neuropathic changes on electrophysiological testing
Animal studies • Animal studies have consistently found that CMV leads to decreased force-generating capacity of the diaphragm
Effects of mechanical ventilation on diaphragmatic contractile properties in rats. Am J Respir Crit Care Med 1994;149(6):1539–1544.
This occurs in a time-dependent manner, • with the force decline becoming evident quite early (within a few days of CMV) • and worsening as mechanical ventilation is prolonged
In-vivo studies • The decrease in diaphragmatic force-generating capacity is not due to changes in lung volume or abdominal compliance • Nervous impulse transmission at the level of the phrenic nerve and the NMJ also remains intact • However, the compound muscle action potential is decreased after CMV • suggesting that impaired muscle fiber membrane excitability and/or excitation–contraction coupling are involved • Effects of prolonged mechanical ventilation and inactivity on piglet diaphragm function. Intensive Care Med 2002;28:358–364.
Isolated diaphragm strip studies • indicate that pathophysiological changes in VIDD are located at the cellular level • diaphragmatic force is normalized for differences in muscle crosssectional area • the loss of force-generating capacity cannot be ascribed to atrophy alone • the diaphragm muscle strip is placed at its optimal length • rules out altered muscle operating length as the major explanation for the force decline
Human studies • more difficult to obtain conclusive proof for the existence of VIDD in humans • multiple confounding factors (e.g., underlying disease state, drug therapy, different modes of mechanical ventilation) • technical limitations in accurately assessing diaphragmatic function in critically ill patients
Histopathologic analysis of 13 neonates • who received ventilatory assistance for 12 days or more immediately before death • revealed diffuse diaphragmatic muscle fiber atrophy, • whereas such changes were not present in • extradiaphragmatic muscles or diaphragms of 26 infants ventilated for 7 days or less • Abnormalities of diaphragmatic muscle in neonates with ventilated lungs. J Pediatr 1988;113:1074–1077.
Abnormalities of diaphragmatic muscle in neonates with ventilated lungs. J Pediatr 1988;113(6): 1074–1077.
in 33 mechanically ventilated but clinically stable patients with a variety of underlying diseases, • the twitch transdiaphragmatic pressure • elicited by supramaximal magnetic stimulation of the phrenic nerves • was found to be reduced by about 50% on average compared with normal subjects • Measurement of twitch transdiaphragmatic, esophageal, and endotracheal tube pressure with bilateral anterolateral magnetic phrenic nerve stimulation in patients in the intensive care unit. Crit Care Med 2001;29:1325–1331.
Twitch transdiaphragmatic pressure measured in mechanically ventilated patients were lower than values reported in ambulatory patients with chronic obstructive pulmonary disease Such marked reduction of the twitch pressure in most of the patients indicates profound respiratory-muscle weakness Assessment of respiratory output in mechanically ventilated patients. Respir Care Clin N Am 2005;11(2):173–199.
Levine et al. evaluated diaphragm biopsy specimens • from adult brain-dead organ donors who had undergone mechanical ventilation prior to organ harvest (18–69 h) • compared with specimens obtained from control patients who were undergoing thoracic surgery for benign lesions or localized lung cancer (mechanical ventilation for 2–3 h) • Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. NEngl JMed2008;358:1327–1335.
biopsy specimens from the organ donor group • a decreased cross-sectional area of slow-twitch and fast-twitch fibers (atrophy), • decreased glutathione levels (suggesting increased oxidative stress), • and greater expression of active caspase-3 and the E3 ubiquitin ligases, atrogin-1, and muscle RING-finger protein-1 (MuRF-1) (implicated in muscle proteolysis) • Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. NEngl JMed2008;358:1327–1335.
Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. NEngl JMed2008;358:1327–1335.
1. Muscle Atrophy • Atrophy develops more rapidly (as early as 18 hours) and to a significantly greater extent in the diaphragm during CMV than in peripheral skeletal muscles • Effects of mechanical ventilation on diaphragmatic contractile properties in rats. Am J Respir Crit Care Med 1994;149(6):1539–1544. • Controlled mechanical ventilation leads to remodeling of the rat diaphragm. Am J Respir Crit Care Med 2002;166:1135–1140.
Atrophy can result from decreased protein synthesis, increased protein degradation, or both • In rats, 6 hours of mechanical ventilation produced a 30% decrease in the rate of mixed muscle protein synthesis and a 65% decrease in the rate of myosin heavy-chain-protein synthesis • Increased protein degradation has been observed in animals exposed to 18 hours of CMV • 3 systems of proteases for intracellular protein degradation: • lysosomal proteases, calpains, and the proteasome system
2. Fiber Remodeling • After 18 hours of CMV, type I (slow-twitch) and type II (fast-twitch) fibers are both decreased in rats, with type II having the greater decrease • the force generated by type I (slow) fibers is less than that of the type II (fast) fibers • decrease in force production by the diaphragm during CMV • Maximum specific force depends on myosin heavy chain content in rat diaphragm muscle fibers. J Appl Physiol 2000;89(2):695–703.
Prolonged duration of CMV (2–4 d), however, results in a different pattern of fiber modification: • a decrease in type I (slow twitch) fibers and an increase in the number of hybrid fibers, which coexpress both slow and fast myosin heavy-chain isoforms. • This change from slow to fast fibers may reduce the endurance of the diaphragm, because fewer slow, fatigue-resistant fibers are available • Principles and practice of mechanical ventilation. New York: McGraw-Hill; 2006.
3.Oxidative Stress • An increase in oxidative stress, reflected by an increase in protein oxidation and lipid peroxidation, has been observed in animals within 6 hours of CMV • Contribute to both muscle atrophy and contractile dysfunction
Antioxidant supplementation attenuates the deleterious effects of CMV on the diaphragm • In critically ill surgical patients, treatment with antioxidant therapy (vitamins E and C) resulted in shorter duration of mechanical ventilation • Randomized, prospective trial of antioxidant supplementation in critically ill surgical patients. Ann Surg 2002;236(6):814–822.
4. Structural Injury • Structural abnormalities of different subcellular components of diaphragmatic fibers have been observed after 48 hours of CMV • disrupted myofibrils, • abnormal swelling of mitochondria, • lipid droplets, • vacuoles
structural alterations in the myofibrils were inversely related to force output of the diaphragm
Mode of Mechanical Ventilation • In a study that compared diaphragmatic function during assist-control ventilation versus CMV • the contractile response of rabbit diaphragm to tetanic stimulation was decreased by 48% after 3 days of CMV • the decrease in force after assist-control ventilation was much less (14%)
Assist-control mechanical ventilation attenuates ventilator-induced diaphragmatic dysfunction. Am J Respir Crit Care Med 2004;170(6):626–632.
Anti-oxidant supplement • the vitamin E analogue Trolox during mechanical ventilation prevents the loss of diaphragmatic contractility and attenuates atrophy in rats • antioxidant supplement containing vitamins E and C was reported to reduce the duration of mechanical ventilation in critically ill patients
Inhibitors of proteolytic pathways • a single administration of leupeptin (inhibitor of calpain/cathepsin) at the onset of mechanical ventilation, not only blocked atrophy, but also prevented intrinsic contractile impairment in the rat diaphragm • Leupeptin inhibits ventilator-induced diaphragm dysfunction in rats. Am J Respir Crit Care Med 2007; 175:1134–1138. • acute high-dose corticosteroid administration was also found to prevent calpain upregulation and mitigate VIDD in rats • Effects of acute administration of corticosteroids during mechanical ventilation on rat diaphragm. Am J Respir Crit Care Med 2008; 178:1219–1226.
inhibition of the proteasome pathway may not be an effective way to prevent the loss of contractile force associated with enhanced proteolysis in the diaphragm • Effect of proteasome inhibitors on endotoxin-induced diaphragm dysfunction. Am J Physiol Lung Cell Mol Physiol 2009; 296:L994–L1001.
Future? • Further research effort required in determining the optimal mode of ventilation to prevent VIDD • ? Other measures designed to target the specific cellular pathways involved in muscle injury • ? how VIDD is influenced by underlying conditions commonly found in mechanically ventilated patients (e.g. sepsis, hyperglycaemia, pre-existing muscle state)
Conclusions • Mechanical ventilation itself may be an important cause of diaphragmatic weakness VIDD • Several factors (e.g., underlying disease state, infection, drug therapy, etc.) can converge with VIDD to exacerbate diaphragmatic weakness in critically ill patients • VIDD – a diagnosis by exclusion of confounding factors
At present, the best approach for preventing VIDD is to avoid controlled mechanical ventilation and the use of neuromuscular blocking agents to the greatest extent possible