Download
1 / 20
200 likes | 601 Views
Hemolytic anemia and Bacillus cereus septicemia in a patient with thalassemia intermedia. Dr Grace Lam April 2010. 45/M Thalassemia intermedia Splenectomy as a child Refused iron chelation therapy Cord compression due to extramedullary hematopoiesis

E N D
Hemolytic anemia and Bacillus cereus septicemia in a patient with thalassemia intermedia Dr Grace Lam April 2010
45/M • Thalassemia intermedia • Splenectomy as a child • Refused iron chelation therapy • Cord compression due to extramedullary hematopoiesis • Clinical admission x Ix of bilateral exudative pleural effusion
Developed fever, respiratory failure & shock • Blood cultures Bacillus species, then –ve • ETA Candida species • Urine Legionella Ag –ve • Mycoplasma Ab <10 • Bilateral pleural fluid: not suggestive of empyema • CT abd & pelvis: possible early liver abscess • Leptospira IgM –ve • Widal test <1:50
Intravascular haemolysis • ↑ Plasma Hb 1900.4mg/L (<50) • ↓ Haptoglobin <0.06 (0.36 - 1.95g/L) • ↑ LDH 457 • Direct antiglobulin test +ve • Anti-IgG +ve • Anti-C3d –ve • Indirect antiglobulin test –ve • Malaria –ve
Treatment • Tienam + Anidulafungin + Doxycycline • Drainage of bilateral pleural effusion • CVVH • High dose vasopressor • Continued to deteriorate despite treatment Δ Septicemia with background thalassemia Waived
Haemolytic anaemia Intravascular haemolysis • RBCs lysed in circulation • Released free Hb: • Bound by serum haptoglobin • Excreted by liver • Filtered into urine • Reabsorbed by renal tubules (Urine haemosiderin) • Haemoglobinuria Extravascular haemolysis • RBCs phagocytosed by macrophages in liver & spleen • Hb broken down & recycled: • Heme → Unconjugated bilirubin • Conjugated in liver • Excreted into GI tract as stercobilinogen
Haemolytic anaemia or normal
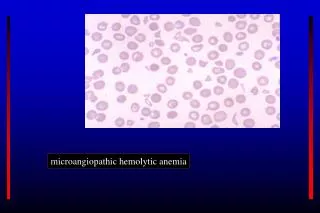
Intravascular haemolysis • Mechanisms • Mechanical trauma • Prosthetic heart valves • Microangiopathic HA (TTP, HUS, DIC, HELLP) • March • Complement fixation • Autoimmune hemolytic anaemia - Cold • Drugs (complement-fixing immune complex) e.g. quinine • Paroxysmal nocturnal haemoglobinuria • Transfusion reactions • Toxic damage
Intravascular haemolysis • Toxic damage • Infections • Clostridium perfringens • Malaria • Babesiosis • Bacillus cereus • Thermal injury • Snake venom • Severe G6PD deficiency
Intravascular haemolysis • Possible cause of intravascular haemolysis in our patient: • +ve Coombs test: Immune-mediated haemolytic anaemia • Toxic damage by infection • Microangiopathic haemolytic anaemia
Direct antiglobulin test • Direct Coombs test • Detects abnormal Ab attached to RBCs • Patient’s RBCs incubated with anti-human antiserum: • Antiserum: Anti-IgG or Anti-C3d (detects complement fixation) -ve = + +ve
Indirect antiglobulin test • Indirect Coombs test • Detects free Ab vs RBCs in serum • Step 1: Incubate patient serum with normal group O RBCs • Step 2: Perform direct antiglobulin test +ve
Coombs test interpretation • Indirect antiglobulin test –ve • Direct antiglobulin test +ve • Anti-IgG +ve • Anti-C3d –ve Warm AIHA Unlikely the cause of intravascular haemolysis without evidence of complement fixation
Coombs test interpretation • Haematopathologist • Strength of +ve Coombs test • Rated on a 4-point scale in PYNEH: + weakest → ++++ strongest • Ag-specificity test on red cell elucidate • Specific red cell Ab: past transfusion • Broad-spectrum Ab: AIHA • Simple bystander as a result of past blood transfusions
Bacillus cereus • A gram +ve or gram-variable bacillus • Produces toxins: Enterotoxin, Hemolysin, Phospholipase C & Emetic toxin • Disease spectrum • Food poisoning in Immunocompetent • Opthalmitis: Post-traumatic, IV drug abuse • Fulminant septicemia in Immunocompromised: MOF, massive intravascular hemolysis, rapid death
Bacillus cereus septicemia • β-lactamase producing • Resistant to Penicillin & Cephalosporin • Carbapenems or Vancomycin • Progressive clinical course despite appropriate antibiotics • ∵ Toxin production Microbiologist: Bacillus circulans (commercial kit) In 1 blood culture only Likely a contaminant
Microangiopathic haemolytic anaemia • Deranged clotting • Platelet DIC – Contribution to intravascular haemolysis
Conclusion • Septicemia in thalassemic patient • Intravascular haemolysis • Contributed by DIC • Positive Coomb’s test • Bystander as a result of past blood transfusions