Download
1 / 18
180 likes | 370 Views
Visual Diagnosis. Sources: 1. Slack Health Care Books, http://www.slackbooks.com 2. Fischer & Vandemark. (1945). J Bone Joint Surg Am.;27:695-698. Pediatrics Morning Report: A 6 week old with direct hyperbilirubinemia. Robyn Rogers, MD Sahar Rooholamini, MD December 9, 2009.

E N D
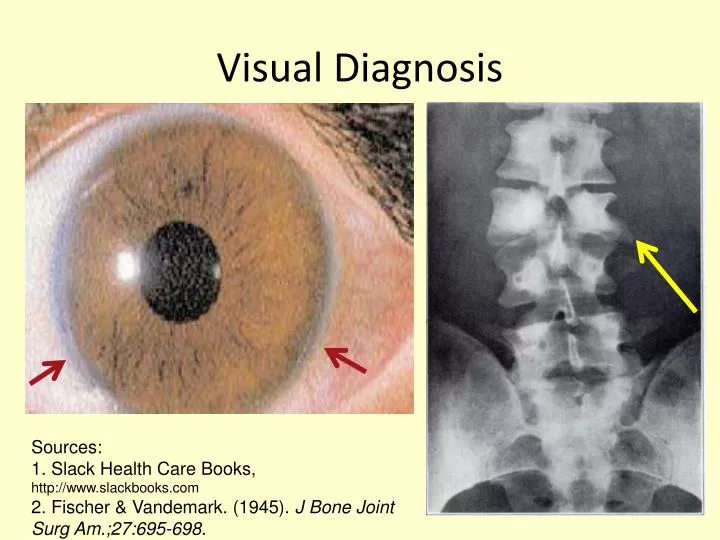
Visual Diagnosis Sources: 1. Slack Health Care Books, http://www.slackbooks.com 2. Fischer & Vandemark. (1945). J Bone Joint Surg Am.;27:695-698.
Pediatrics Morning Report:A 6 week old with direct hyperbilirubinemia Robyn Rogers, MD Sahar Rooholamini, MD December 9, 2009
Case Presentation • You’re the Green Team (GI) resident and you’re called to admit a patient. • You’re told: “This is a 6 week old male from an outside hospital who has direct hyperbilirubinemia and needs a work-up.” • What is your initial differential diagnosis? • What do you want to know?
Learning Objectives • Generate and understand the differential diagnosis for conjugated hyperbilirubinemia in an infant • Understand the essential elements of the history and physical in conjugated hyperbilirubinemia • Learn the general diagnostic and therapeutic approaches to conjugated hyperbilirubinemia
Physiologic vs. Non-physiologic Jaundice Physiologic Non-physiologic Variety of causes Present at birth or persistent beyond 2 weeks of life Conjugated hyperbilirubinemia is a potential RED FLAG at any age and requires follow-up Associated with other signs or symptoms • Caused by structural and functional immaturity of neonatal hepatobiliary system • Almost always unconjugatedhyperbilirubinemia • Expected to resolve by 2 weeks of life • Ex: breastfeeding and breast milk jaundice
Definitions and Epidemiology • Conjugated hyperbilirubinemia = Serum direct bili > 1 mg/dL (if total bili <5 mg/dL), or > 20% of total bilirubin • AKA “neonatal cholestasis” • Affects 1 in 2500 births • Most common causes: • Neonatal Hepatitis 70-80% of cases, • Biliary Atresia usually term infants • Alpha-1 Antitrypsin Deficiency • 10-15% of cases
Bilirubin conjugation and excretion Bloomer J (2006). Gastroenterology and Hepatology: Liver. Edited by Mark Feldman (series editor). Published by Current Medicine Group. Obtained through Lane Medical Library.
Differential Diagnosis of Conjugated Hyperbilirubinemia • Anatomic approach • Intrahepatic vs. extrahepatic causes • Physiologic approach • Impaired bile formation (hepatocyte problem) vs. obstruction to bile flow (either within or outside liver)
Impaired bile formation • Acute liver damage (hypoxia, ischemia, acidosis) • Infection/sepsis • Bacterial: E. coli, GBS, Listeria, TB, syphilis • Viral: HIV, hepatitides, Rubella, CMV, HSV • Parasitic: Toxoplasma • Genetic/Metabolic diseases (abbreviated list) • Alpha-1 antitrypsin deficiency • IEM: Galactosemia, tyrosinemia; lipid and bile salt metabolic defects • Cystic Fibrosis • Endocrine disorders (hypothyroidism, hypopituitarism) • Toxin or Drug-induced damage • TPN-related liver disease • Idiopathic Neonatal Hepatitis (dx of exclusion)
Obstruction to Bile Flow • Congenital anomalies • Biliary atresia • Choledochal cyst • Alagille syndrome (paucity of intrahepatic bile ducts) • Bile duct stenosis • Other anatomic anomalies • Bile duct perforation or compression • Cholelithiasis/sludging
History & Physical • Family history • Prenatal, neonatal hx • Dietary hx, weight gain • Stooling pattern, color • Urine color • History of bruising or bleeding • Irritability, seizures • VS and growth parameters • Neurologic exam (e.g., tone, symmetry, reflexes) • Eye exam • Dysmorphic features • Jaundice • Heart murmur • Hepatosplenomegaly • Bruising/petechiae • Urine and stool
Initial Work-Up • A thorough H&P should guide subsequent testing. • Total/direct bilirubin • Transaminases, Alkaline phosphatase, GGT • Synthetic liver function tests (coags, albumin) • UA, Ucx; blood and CSF cultures if indicated • CBC with reticulocyte count • Hepatitis panel, TORCH titers • TSH, Free T4 • Serum Alpha 1-AT level +/- phenotype • Sweat chloride • Serum and urine organic/amino acids
Further Work-Up & Imaging • Ultrasound • Keep patient NPO • Try to feed during exam to show gallbladder contraction • Hepatobiliary scintigraphy (HIDA scan) • Perform after 3-5 days of phenobarbital to promote bile flow, at 5 mg/kg/day • Duodenal aspirate • MRCP/ERCP (not routinely recommended) • Liver biopsy
Additional Case History • Patient’s test results and hospital course • Post-discharge follow-up • This patient was initially admitted for a liver biopsy for concern for biliary atresia…would you have biopsied him?
Management of Conjugated Hyperbilirubinemia • Medical Management • Phenobarbital • Ursodiol • Rifampin • Cholestyramine • Diet • Medium-chain triglycerides • Fat-soluble vitamin supplementation • Surgical interventions • Kasai portoenterostomy • Liver transplantation
Summary and Take-Home Points • Maintain a healthy skepticism about the working diagnosis on all of your patients. • Approach conjugated hyperbilirubinemia with a broad differential diagnosis but focused work-up. • A patient with jaundice persisting beyond 2-3 weeks of age needs further work-up, beginning with total and direct bilirubin measurements.
Thank you, Drs. Kerner and Fuentebella!References Fischer & Vandemark (1945). Sagittal Cleft (Butterfly) Vertebra. Journal of Bone and Joint Surgery; 27:695-698. NASPGHAN (2004). Guideline for the Evaluation of Cholestatic Jaundice in Infants. Journal of Pediatric Gastroenterology and Nutrition; 39:115–128. Slack Health Care Books. Posterior Embryotoxon (image). http://www.slackbooks.com. Venigalla & Gourley (2004). Neonatal cholestasis. Seminars in Perinatology; 28:348-355. More clinical guidelines can be found here: http://www.naspghan.org/