Download
1 / 49
490 likes | 694 Views
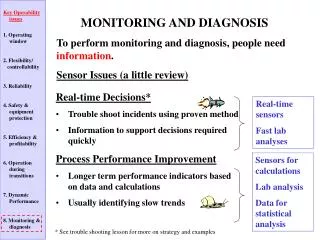
The use of antineutrophil antibodies in the diagnosis and monitoring of small vessel vasculitis. Critically Appraised Topic Steven Vervaeke 19 - 04 - 2005. ANCA. A nti- N eutrophil C ytoplasmic A ntibodies. ANCA. hυ’. hυ. c-ANCA : C ytoplasmatisch Diffuus, granulair,

E N D
The use of antineutrophil antibodies in the diagnosis and monitoring of small vessel vasculitis Critically Appraised Topic Steven Vervaeke 19 - 04 - 2005
ANCA Anti-Neutrophil Cytoplasmic Antibodies
hυ’ hυ
c-ANCA: Cytoplasmatisch Diffuus, granulair, cytoplasmatisch patroon.
p-ANCA: Perinucleair Perinucleaire tot nucleaire aankleuring.
De termen p-ANCA en c-ANCA slaan op het immuunfluorescentiepatroon!
Ethanol- en Formaline-fixatie van testgranulocyten. ETHANOL:invloed op spreiding van Ag, sommige migreren richting kern en zijn verantwoordelijk voor het p-ANCA patroon GEVOLG: kans op verwarring met ANA-patroon. FORMALINE: geen Ag-migratie.
C-ANCA Proteinase 3 (PR3) BPI (CAP-57) andere onbekende Ag P-ANCA Myeloperoxidase (MPO) Lactoferrine Elastase BPI (CAP-57) Cathepsin G β-glucuronidase Lysozyme α-enolase ... Target-antigenen
C-ANCA M. Wegener (80-90%) MPA (10-35%) CSS (10-20%) PAN (< 5%) P-ANCA Primaire vasculitis: MPA (42-70%) CSS (18-60%) WG (10%) Andere: SLE RA IBD Chronische leverziekten ... Ziekte-associatie
VAN ALLE ANTIGENEN ZIJN ENKEL MPO EN PR3 GEASSOCIEERD MET PRIMAIRE VASCULITIS. GEEN ENKEL ANDER ANTIGEN HEEFT EEN DIAGNOSTISCHE BETEKENIS BIJ GEEN ENKELE ANDERE AANDOENING!
ELISA MPO of PR3
ELISA Serum patient met ANCA
ELISA MPO of PR3-ANCA
De termen MPO-ANCA en PR3-ANCA slaan op ANCA specifiek gericht tegen MPO of PR3 (ELISA)
IIF: Primaire vasculitis of niet? Problemen: - Echte p-ANCA of ANA of beide? - Indien p-ANCA: welk antigen?
TEST GUIDELINES: Een positieve IIF test moet steeds bevestigd worden door een MPO of PR3 positieve ELISA.
Ziekte-associatie van de gecombineerde IIF en ELISA test IIF patroon Antigen Ziekte C-ANCA PR3 WG (80-90%) MPA (20-40%) CSS (35%) P-ANCA MPO MPA (50%) CSS (35%) WG (10%)
ANCA-geassocieerde vasculitiden • Morbus Wegener: • Prevalentie: 3 per 100.000 • Microscopische polyangiitis: • Incidentie: 1 per 100.000 per jaar • Churg-Strauss syndroom: • Incidentie: 1 tot 3 per 1.000.000 per jaar
Diagnostische waarde vd testen (Hagen et al. 1998) Wegener MPA Sensitiviteit: c-ANCA 64% 23% p-ANCA 21% 58% PR3 66% 26% MPO 24% 58% Specificiteit tov zieke controles: c-ANCA 95% PR3 87% p-ANCA 81% MPO 91%
Diagnostische waarde vd testen (Hagen et al. 1998) Wegener MPA Sensitiviteit: c-ANCA + PR3 57% p-ANCA + MPO 49% beide 73% 67% Specificiteit tov zieke controles: 99%. Gezonde controles: 100%
Diagnostische waarde vd testen (Hagen et al. 1998) CONCLUSIE: De waarde van de IIF test voor ANCA kan gevoelig verhoogd worden door ze te combineren met ELISA.
Diagnostische waarde vd testen (Hagen et al. 1998) CONCLUSIE: C-ANCA + PR3 is kenmerkend voor WG p-ANCA + MPO is kenmerkend voor MPA Niet alle IIF ANCA positieven zijn AAV pat. Niet alle AAV patienten testen positief
Indicaties voor gebruik van ANCA in diagnostiek: • Edgar et al., 1995: • Slechts 27% van alle ANCA-aanvragen gebeuren in kader van een AAV. • AAV zijn zeldzame aandoeningen • Hoge vals-positiviteit: • ANCA komen in tal van ziektes voor. • ANA • ANCA zijn niet essentieel in de diagnose van AAV (classificatiecriteria)
Indicaties voor gebruik van ANCA in diagnostiek: • International consensus statement on testing and reporting of ANCA (1999): • Glomerulonefritis • Longbloeding • Cutane vasculitis met systemische weerslag • Meerdere longnoduli • Chronische destructieve BLW pathologie • Chronisch actieve sinusitis of otitis • Subglottische trachea stenose • Mononeuritis multiplex of andere perifere neuropathie • Retro-orbitale massa • indien er geen andere duidelijke oorzaak voor is !
Indicaties voor gebruik van ANCA in diagnostiek: • CSS? • Asthma, eosinofilie en vasculitis. • Koorts, arthralgie, myalgie, vermoeidheid? • GEEN INDICATIES! • ANCA is geen screeningstest! • Maar: • AAV vaak moeilijke diagnose • elke ernstige, acute pathologie (vooral wanneer longen en/of nieren betrokken) heeft recht op een ANCA-test.
Aanvraaggedrag ANCA in UZ Leuven: • April 2003 - Oktober 2004: 7781 aanvragen • 6391 (82,1%) negatief op IIF • 911 (11,7%) positief op IIF • 479 (6,2%) dubieus op IIF • 597 aanvragers: • aanvraagfrequentie: 1 per 1,5 jaar tot 21 aanvragen per maand.
Aanvraaggedrag ANCA in UZ Leuven: % IIF positief % ELISA positief aantal Pos. Pos.+Dub IIF Pos. IIF Dub. IAL 1245 14,5 21,9 49 (56) 15 (22) NEU 638 3,1 7,1 15 (16) 0 (12) NEF 585 13,9 18,8 42 (56) 10 (28) HEP 450 10,7 16,5 6 (19) 12 (15) REU 374 24,6 32,916 (28) 3 (6) PNE 345 9,6 16,3 27 (36) 4 (8) GE 212 17 22,7 NB NB ALL 203 2,9 5,8 NB NB NKO 107 4,7 7,4 NB NB GER 63 6,3 14,2 NB NB PED 52 11,5 13,5 NB NB HEM 34 5,8 14,7 NB NB
Filter op de aanvragen? • Werkt het systeem? • Sinclair et al. 2004: • Criteria opgesteld (~ ICG) • 72,5% vd aanvragen werd toegelaten tot de test • Resultaat van de aanvaarde aanvragen • 73% negatief • 27% positief waarvan 74% inderdaad AAV patienten. • Slechts 1 patient vd geweigerde patienten ontwikkelde een AAV in de follow-up (delay 2 dagen) • CONCLUSIE: het selecteren van aanvragen heeft een positieve impact op de test: klinische relevantie van een positieve test stijgt en de procedure werkt kostensparend.
Filter op de aanvragen? • Werkt het systeem? • Mandl et al. 2004:
Filter op de aanvragen? • Werkt het systeem? • Mandl et al. 2004: • Retrospectieve studie • Het aantal ANCA-testen zou met 23% zakken • Het aandeel van de vals positieve IIF zou zakken met 27% • Geen enkele AAV werd gemist. • Noot: neurologie PPV: 0%! • CONCLUSIE: het toepassen van selectiecriteria op ANCA-aanvragen zorgt voor een efficiënter gebruik van de test en voor een gevoelige kostenbesparing in het labo.
Filter op de aanvragen? • Werkt het systeem? • UZ Gasthuisberg: • Retrospectieve studie over 18 maand op IAL. • 286 aanvragen: • Negatieve IIF: 199 (69,5%) • 78 aanvragen zouden aanvaard worden (39%) • Positieve IIF: 56 (19,5%) • 32 aanvragen zouden aanvaard worden (57%) • Dubieuze IIF: 31 (11%) • 16 aanvragen zouden aanvaard worden (52%) • GEEN ENKELE AAV WERD GEMIST!
Filter op de aanvragen? • Werkt het systeem? • UZ Gasthuisberg: • Op totaal van 286 aanvragen werd 44% toegelaten. • Per jaar: • Ongeveer 5500 aanvragen • 21 500 euro minstens uitgespaard per jaar voor IIF • Kosten voor een positieve IIF niet ingecalculeerd. • ANCA voor IBD en AIH als ‘niet geaccepteerd’.
Filter op de aanvragen? • Werkt het systeem? • Slecht of onvolledig ingevulde ‘klinische inlichtingen’ • Wie doet het werk? • Electronische aanvraag en ‘vasculitis screening’ • Wat met een gemiste diagnose tgv niet aanvaarden van de aanvraag.
ANCA in de follow-up van AAV • Therapie niet zonder risico • Herval niet zonder risico • Een merker die een AAV-herval kan aangeven? • ANCA rol in pathogenese van AAV • Patienten in remissie: ANCA vaak niet meer detecteerbaar. • Actieve Wegener: hogere titers dan andere patienten
ANCA in de follow-up van AAV • Literatuur: controversieel. • Stegeman, 2002: • Meeste studies ‘minderwaardig’ • Correct opgezette studies: • 4-voudige toename van c-ANCA titer op IIF OF • > 75% toename in PR3-ANCA op ELISA is in meer dan 50% van de gevallen geassocieerd met een herval binnen de 6 tot 12 maand. (Wegener)
ANCA in de follow-up van AAV • Girard et al. 2001: • Herverschijnen van ANCA bij AAV patienten slechts in 37% geassocieerd met herval. • Persisterende positiviteit was in 31% van de gevallen geassocieerd met herval. • De delay tussen ANCA stijging en herval kan heel lang zijn (maanden). • CONCLUSIE: er is een verband, doch zwak. Niet voldoende om behandeling te wijzigen. ANCA stijging is een waarschuwingssignaal.
Verder doel van de CAT: • Wat met onze flow-chart? • Mogelijke problemen: • ‘Dubieus’ op titer 1/40 • Dubbele stalen op ELISA • Cut-off MPO-ELISA: • Onze cut-off: 5 U (firma: 20 U) • Geteste populatie: 50 stalen met ‘IIF pos.’ en ‘MPO’ • 18 op 50 hadden MPO tussen 5 U en 20 U: • Slechts 3 waren geassocieerd met AAV • 32 op 50 hadden MPO boven 20 U: • 16 AAV en 13 andere vasculitiden (29 op 32)
Verder doel van de CAT: • Cut-off MPO-ELISA: • Cut-off > 20 U: 16 AAV op 32 stalen (50%) • Cut-off > 5 U: 19 AAV op 32 stalen (38%) • Cut-off > 20 U: Sensitiviteit: 53% - specificiteit 99% • Cut-off > 5 U: sensitiviteit: 100% - specificiteit 0%
ANCA praktisch • Preanalytisch: • serum, 2-8°C. • Geen gehemolyseerde, besmette, onvolledig gedefibrineerde,… stalen: achtergrond kleuring • Reproduceerbaarheid: • IIF: interassay en interobserver variation • ELISA: te bekijken
ANCA praktisch • Diagnostische performantie: • IIF IAL: sensitiviteit 68%, specificiteit 80% (zieken)
ANCA praktisch • TAT: • < 10 dagen. • IIF: vier maal per week (niet op woensdag) • ELISA: twee maal per week (dinsdag en vrijdag)
ANCA praktisch • Kosten: • IIF: • Consumable cost: 4,34 euro • TU and Log: 1,73 euro • Support: 1,79 euro • Invest: 0 euro • TOTAAL: 7,86 euro. • Extra: elke titratiestep herhaalt deze kost. • ELISA: • Consumable cost: 15,65 euro • TU and Log: 2,84 euro • Support: 2,80 euro • Invest: 0,12 euro • TOTAAL: 2 x 21,47 = 42,94 euro
ANCA praktisch • Terugbetaling: • IIF: • ANCA-detectie: B300 = 8,4 euro • ANCA-titratie: B400 = 11,20 euro • Totale terugbetaling voor positieve IIF: B700 = 19,60 euro Noot: kosten kunnen oplopen tot 47,16 euro ! • ELISA: • PR3 detectie: B350 = 9,80 euro • MPO detectie: B350 = 9,80 euro • Totale terugbetaling voor ELISA: B700 = 19,60 euro. Noot: kostprijs ELISA bedraagt 42,94 euro! • Dus: om de kosten van één vals positief IIF resultaat te compenseren zijn 36 tot 94 negatieve stalen nodig!
To Do’s: • Overleg met clinici mbt de selectiecriteria voor ANCA-testen. • Afwerken statistische analyse op onze ANCA-aanpak. • Bijstellen cut-off waarden ELISA • Aanpassen flow-chart • Zin of onzin van het in duplo lopen van stalen op de ELISA. • ANCA-testen voor ander doeleinden dan AAV?
Om te onthouden: “The problems of antineutrophil cytoplasmic antibody testing include the diversityof antineutrophil cytoplasmic antibody target antigens, assay standardisation and performance, the application of antineutrophil cytoplasmic antibody testing in a clinical setting with a low pretest probability, and, finally, the widespread assumption that antineutrophil cytoplasmic antibody titers alone may closely reflect disease activity and therefore may be used to guide therapy. Recent findings demonstrate that the combined use of indirect immunofluorescence tests and solid phase assays to detect antineutrophil cytoplasmic antibody directed against myeloperoxidase and proteinase 3 can minimize the occurrence of false-positive antineutrophil cytoplasmic antibody results. Furthermore, the yield of antineutrophil cytoplasmic antibody testing can be improved by the use of a well standardised test, adherence to published guidelines, and restricting the use of the test to clinical situations with a rather high pretest probability for antineutrophil cytoplasmic antibody-associated vasculitides. However, treatment decisions should be based on the clinical presentation of the patient and histological findings and not on the results of antineutrophil cytoplasmic antibody testing alone.” Schmitt and van der Woude, 2004.