Download
1 / 1
10 likes | 159 Views
No. 206. Superficial bladder c ancer : Time from diagnosis to first tumour recurrence ). Dr Rachel Jackson, Mr Richard Grills, Mr Stephen Lane Urology Unit, The Geelong Hospital, Barwon Health, Victoria Australia. Posters Proudly Supported by: . Introduction

E N D
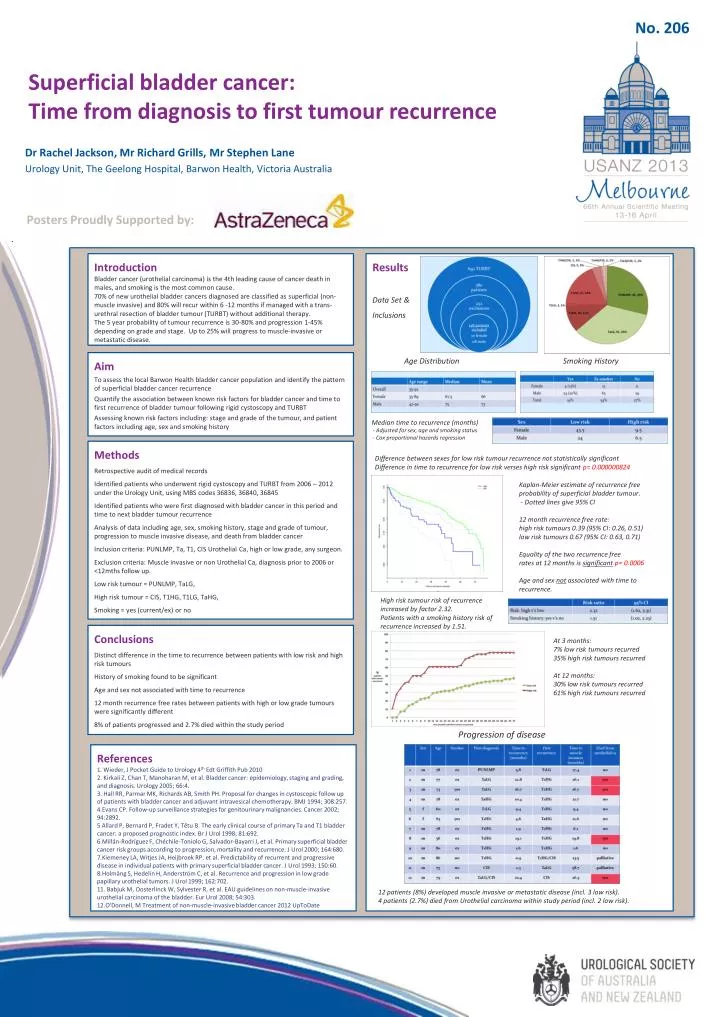
No. 206 Superficial bladder cancer: Time from diagnosis to first tumour recurrence) Dr Rachel Jackson, Mr Richard Grills, Mr Stephen Lane Urology Unit, The Geelong Hospital, Barwon Health, Victoria Australia Posters Proudly Supported by: Introduction Bladder cancer (urothelial carcinoma) is the 4th leading cause of cancer death in males, and smoking is the most common cause. 70% of new urothelial bladder cancers diagnosed are classified assuperficial (non-muscle invasive)and 80% will recur within 6 -12 months if managed with a trans-urethral resection of bladder tumour (TURBT) without additional therapy. The 5 year probability of tumour recurrence is 30-80% and progression 1-45% depending on grade and stage. Up to 25% will progress to muscle-invasive or metastatic disease. Results Data Set & Inclusions Age Distribution Smoking History Aim To assess the local Barwon Health bladder cancer population and identify the pattern of superficial bladder cancer recurrence Quantify the association between known risk factors for bladder cancer and time to first recurrence of bladder tumour following rigid cystoscopy and TURBT Assessing known risk factors including: stage and grade of the tumour, and patient factors including age, sex and smoking history Median time to recurrence (months) - Adjusted for sex, age and smoking status - Cox proportional hazards regression Methods Retrospective audit of medical records Identified patients who underwent rigid cystoscopy and TURBT from 2006 – 2012 under the Urology Unit, using MBS codes 36836, 36840, 36845 Identified patients who were first diagnosed with bladder cancer in this period and time to next bladder tumour recurrence Analysis of data including age, sex, smoking history, stage and grade of tumour, progression to muscle invasive disease, and death from bladder cancer Inclusion criteria: PUNLMP, Ta, T1, CIS UrothelialCa, high or low grade, any surgeon. Exclusion criteria: Muscle invasive or non UrothelialCa, diagnosis prior to 2006 or <12mths follow up. Low risk tumour = PUNLMP, TaLG, High risk tumour = CIS, T1HG, T1LG, TaHG, Smoking = yes (current/ex) or no Difference between sexes for low risk tumour recurrence not statistically significant Difference in time to recurrence for low risk verses high risk significant p= 0.000000824 • Kaplan-Meier estimate of recurrence free • probability of superficial bladder tumour. • - Dotted lines give 95% CI • 12 month recurrence free rate: • high risk tumours 0.39 (95% CI: 0.26, 0.51) • low risk tumours 0.67 (95% CI: 0.63, 0.71) • Equality of the two recurrence free • rates at 12 months is significantp= 0.0006 • Age and sex not associated with time to recurrence. High risk tumour risk of recurrence increased by factor 2.32. Patients with a smoking history risk of recurrence increased by 1.51. Conclusions Distinct difference in the time to recurrence between patients with low risk and high risk tumours History of smoking found to be significant Age and sex not associated with time to recurrence 12 month recurrence free rates between patients with high or low grade tumours were significantly different 8% of patients progressed and 2.7% died within the study period At 3 months: 7% low risk tumoursrecurred 35% high risk tumours recurred At 12 months: 30% low risk tumours recurred 61% high risk tumours recurred Progression of disease References 1. Wieder, J Pocket Guide to Urology 4thEdt Griffith Pub 2010 2. Kirkali Z, Chan T, Manoharan M, et al. Bladder cancer: epidemiology, staging and grading, and diagnosis. Urology 2005; 66:4. 3. Hall RR, Parmar MK, Richards AB, Smith PH. Proposal for changes in cystoscopic follow up of patients with bladder cancer and adjuvant intravesical chemotherapy. BMJ 1994; 308:257. 4.Evans CP. Follow-up surveillance strategies for genitourinary malignancies. Cancer 2002; 94:2892. 5 Allard P, Bernard P, Fradet Y, Têtu B. The early clinical course of primary Ta and T1 bladder cancer: a proposed prognostic index. Br J Urol 1998; 81:692. 6.Millán-Rodríguez F, Chéchile-Toniolo G, Salvador-Bayarri J, et al. Primary superficial bladder cancer risk groups according to progression, mortality and recurrence. J Urol 2000; 164:680. 7.Kiemeney LA, Witjes JA, Heijbroek RP, et al. Predictability of recurrent and progressive disease in individual patients with primary superficial bladder cancer. J Urol 1993; 150:60. 8.Holmäng S, Hedelin H, Anderström C, et al. Recurrence and progression in low grade papillary urothelial tumors. J Urol 1999; 162:702. 11. Babjuk M, Oosterlinck W, Sylvester R, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder. EurUrol 2008; 54:303. 12.O'Donnell, M Treatment of non-muscle-invasive bladder cancer 2012 UpToDate 12 patients (8%) developed muscle invasive or metastatic disease (incl. 3 low risk). 4 patients (2.7%) died from Urothelial carcinoma within study period (incl. 2 low risk).