Download
1 / 38
430 likes | 745 Views
Chronic Respiratory diseases. By Prof. Asmaa Abdul Aziz. Chronic respiratory diseases are one of the categories of Chronic diseases which represent a big portion of death . These are : Cardiovascular diseases 30 % Cancer 13 % Chronic Respiratory diseases 7 % Diabetes 2 %

E N D
Chronic Respiratory diseases By Prof. Asmaa Abdul Aziz
Chronic respiratory diseases are one of the categories of Chronic diseases which represent a big portion of death . These are : • Cardiovascular diseases 30 % • Cancer 13 % • Chronic Respiratory diseases 7 % • Diabetes 2 % • Epidemic of chronic diseases is neglected because: • 1-Reduction of Chronic diseases is not a Millennium Goal • 2The emphases of some infectious diseases ( HIV, TB, Malaria ) is more than that for chronic diseases. • The prevalence of chronic pulmonary diseases is under- estimated because of the ways of the cause of death were classified . Usually the focus is on the heart , cancer and stroke because they are concluded as the major cause of death. Dr. Asmaa 2009
COPD is sometimes referred to as emphysema or chronic bronchitis • COPD is a serious lung disease that over time, makes it hard to breathe – long term condition • Healthy airways and air sacs in the lungs are elastic . Loss of elasticity, makes it hard to get air in and out What is COPD? Dr. Asmaa 2009
Constant coughing, sometimes called "smoker's cough" • Shortness of breath while doing activities, • Excess sputum production, frequent chest infections • Dyspnoea • Wheezing • COPD are progressive, develops slowly, and can worsen over time What are the symptoms? Dr. Asmaa 2009
Key Indicators for Considering a Diagnosis of Chronic Obstructive Pulmonary Disease • Indicator Characteristics • Chronic cough Present intermittently or every day • Often present throughout the day; seldom only • nocturnal • Chronic sputum production Any pattern of chronic sputum production may indicate • COPD • Dyspnea : Progressive (worsens over time) • Persistent (present every day) • Described by the patient as “increased effort to breath,” • “heaviness,” “air hunger,” or “gasping” • Worse on exercise & respiratory infection • History of exposure to Tobacco smoke • risk factors, especially: Occupational dusts and chemicals • Smoke from home cooking and heating fuels Dr. Asmaa 2009
Test for COPD is called Spirometry • Simple, non-invasive breathing test that measures the amount of air a person can blow out of the lungs (volume) and how fast he or she can blow it out (flow) • Results will indicate presence of COPD & severity • The spirometer measures • the total amount exhaled, called the forced vital capacity (FVC), and • how much you exhaled in the first second, called the forced expiratory volume in 1 second (FEV1) How are you tested for COPD? • Classification • mild COPD 50% to 80% FEV1 • moderate COPD 30% to 50% FEV1 • severe COPD Less than 30% FEV1 Dr. Asmaa 2009
COPD Versus Asthma COPD ASTHMA • Onset in mid-life ( above 40) • Symptoms slowly progressive • Dyspnea during exercise • irreversible airflow limitation • Onset early in life (often childhood) • Symptoms vary from day to day • Symptoms at night/early morning • Allergy, rhinitis, and/or eczema • Family history of asthma • reversible airflow limitation Dr. Asmaa 2009
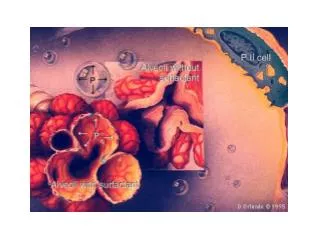
The role of α1 antitrypsin inhibitor • The alveoli are elastic . • Neutrophil elastase is a proteolytic enzyme destroys the alveolar wall • Normally α1 antitrypsin inhibitor produced in the liver and carried by the blood to the lung .It inhibits the action of the elastase so keeps the elasticity. • Hereditary deficiency of α1 antitrypsin inhibitor makes the alveoli losses their elasticity • Non smokers below the age of 40 years suffering from emphysema have hereditary deficiency of α1 antitrypsin inhibitor Dr. Asmaa 2009
There are three mechanisms for the limitations of air flow in the small air ways : • Loss of elasticity of the alveoli and the small air ways • Inflammation cause narrowing of the small airways • Mucous secretion which block the air ways Dr. Asmaa 2009
Smoking is the most common cause of COPD- out of 10 deaths from COPD 9 are smokerssmoking (either current or former smokers) Who is at risk? • Long-term exposure to irritants ( chemicals, dust, or fumes in the workplace). • Heavy or long-term exposure to indoor or outdoor air pollutants • COPD is caused by a genetic condition known as alpha-1 antitrypsin, (AAT), deficiency. People with AAT deficiency can get COPD without above exposures Dr. Asmaa 2009
stress • Sex • Age :COPD is common >40yrs with history of smoking • Respiratory infections • Socioeconomic status • Nutrition • Comorbidities Who is at risk?Cont. Dr. Asmaa 2009
Changes in Lung Parenchyma in COPD Alveolar wall destruction Loss of elasticity Destruction of pulmonary capillary bed ↑ Inflammatory cells macrophages, lymphocytes Dr. Asmaa 2009
The prevalence of COBD: • The global prevalence of COPD for persons 40 years or older is 9 to 10%, and is higher in smokers than in nonsmokers, and higher in men than in women. • High prevalence in low income countries than that in high income countries • Gender Differences • COPD are Smoking-related diseases continuing to increase among women in the United States, while they have plateaued or are decreasing among men. • Compared with men at a similar level of tobacco smoking, women may be more likely to develop COPD or that the severity of COPD in women may be increased
COPD Mortality by Gender,U.S., 1980-2000 Men Women Number Deaths x 1000 1980 1985 1990 1995 2000 Source: US Centers for Disease Control and Prevention, 2002 Dr. Asmaa 2009
Of the six leading causes of death in the United States, only COPD has been increasing steadily since 1970 Dr. Asmaa 2009 Source:Jemal A. et al. JAMA 2005
Causes of Death in Patients with COPD Rabe K. N Engl J Med 2007;356:851-854 Dr. Asmaa 2009
COPD and CMorbidities • COPD patients are at increased risk for: • Myocardial infarction, angina • Osteoporosis • Respiratory infection • Depression • Lung cancer • Weight loss • Nutritional deficiency • Skeletal muscle dysfunction Dr. Asmaa 2009
Exacerbation of COPD • “An event in the natural course of the disease characterized by a change in the patient’s baseline dyspnea, cough, and/or sputum that is beyond normal day-to-day variations, is acute in onset. • Exacerbation frequency increases with increase in disease severity and is associated with poorer health outcomes • The most common causes of an exacerbation are infection of the tracheobronchial tree and air pollution, or change in regular medication but the cause of one-third of exacerbations cannot be identified • Patients COPD exacerbations with clinical signs of airway infection (e.g., increased sputum purulence) will benefit from antibiotic treatment. Dr. Asmaa 2009
Management of Stable COPD • Avoidance of risk factors • smoking cessation • reduction of indoor pollution • reduction of occupational exposure • Influenza vaccination • Pneumococcal vaccination Dr. Asmaa 2009
Management of COPD : 1- Bronchodilators 2-Corticosteroid 3- Antibiotics : should be given during exacerbation & should be given in acute episode ( as soon as the sputum turns yellow ) to prevent further lung damage 4- Diuretics for all edematous patients 5- α Antitrypsin replacement for patients with serum level of this compound below 310 mg / L and abnormal lung functions Dr. Asmaa 2009
Measures for Stable COPD :Vaccines • In patients with COPD the ,symptoms are worsened if they get influenza , so Influenza vaccines can reduce serious illness • Pneumococcal polysaccharide vaccine is recommended for: • COPD patients 65 years and older and • COPD patients younger than age 65 with an FEV1 < 40% predicted Dr. Asmaa 2009
Pneumococcal vaccine can preventillness caused bystreptococcus pneumoniae, such as : • pneumonia, • bronchitis • meningitis • septicemia • ear infections. • In general the Pneumococcal vaccine should be given to • elderly having: COPD , Liver diseases, Diabetes mellitus • Children with haemoglobinopathies & Congenital heart • There are two types of Pneumococcal vaccine: • 1- Pneumococcal polysaccharide vaccine (PPV) • 2-Pneumococcal conjugate vaccine (PCV) Dr. Asmaa 2009
1- Pneumococcal polysaccharide vaccine (PPV) Inactivated ,contains purified capsular polysaccharide from each of 23 serotypes of Pneumococcal bacteria 2-Pneumococcal conjugate vaccine (PCV) contains Inactivated capsular polysaccharide from seven serotypes of Pneumococcal bacteria conjugated to protein The vaccines are inactivated, do not contain live organisms and cannot cause the diseases against which they protect. Dr. Asmaa 2009
Pneumococcal polysaccharide vaccine (PPV) • Adults develop a good antibody response to a single dose of PPV by the third week following immunization. • Not used in children < two years of age because of poor antibody responses . • The overall efficacy is 50 to 70% • Post-immunization antibody levels begin to wane after five years Dr. Asmaa 2009
Pneumococcal conjugate vaccine (PCV) • The antibody response in young children can be improved by conjugating the polysaccharide to proteins. • The conjugated vaccine is immunogenic in children • The efficacy is 97% after the fourth dose • The vaccine protects against Pneumococcal meningitis, bacteraemia, pneumonia and otitis media. • For children under one year of age: • Four doses ( 0.5ml each) of PCV at 2nd, 4th of 6th month • The fourth dose of 0.5ml at 13th month • Subcutaneous at anterolateral thigh • ForChildren from 1-5 year of age • A single dose of 0.5ml of PCV (subcutaneous upper arm) Dr. Asmaa 2009
Contraindications : • Don’t give the conjugate PCVvaccine to children had a serious (life-threatening) allergic reaction to a previous dose of this vaccine ( as it contains protein) • Postponed the PCV vaccine for children who are severely ill .Wait until they recover before getting the vaccine Dr. Asmaa 2009
The PCV vaccine could be given to Children even with minor illnesses, such as mild fever or diarrhea • Adverse effects following PCV • 25% had local redness, tenderness, or swelling • • Up to about 1 out of 3 had a fever • • Some persons become drowsy, or had anorexia Dr. Asmaa 2009
Chronic Tonsillar diseases These are recurrent/chronic infection, hyperplasia of the tonsils Most common organisms cultured from patients with chronic tonsillar disease is • Streptococcus pyogenes (Group A beta-hemolytic streptococcus) Followed by: • Haemophilus influenza • Staphylococcus aureus • Streptococcus pneumonia Tonsil weight is directly proportional to bacterial load. Dr. Asmaa 2009
4 or more episodes of group A streptococcal infections per year results in chronic tonsillitis. The repeated attack is due to: • poor compliance with treatment • new infection from a close contact Dr. Asmaa 2009
Streptococcal infections are either Respiratory or None respiratory 1-Respiratory: A- Acute Streptococcal Pharyngitis or Tonsillitis: Asymptomic individuals represent 20-40% ( carrier) The symptoms typically are : sudden onset of fever, sore throat, malaise, anorexia, tender and enlarged anterior cervical lymph nodes, exudative tonsillitis or pharyngitis as well as congestion and edema of the pharynx and tonsils. B-Scarlet fever: Scarlet fever patients have all signs and symptoms of streptococcal pharyngitis or tonsillitis & the characteristic rash & strawberry tongue The rash occurs due to toxins that spread through the blood. 2-Nonerespiratory: Puerperal sepsis , impetigo , cellulites , wound infections Dr. Asmaa 2009
Streptococcal Pharyngitis &Tonsillitis: Dr. Asmaa 2009
Complications of respiratory streptococcal diseases A)The suppurative peritonsillar abscess, cervical adenitis, purulent rhinitis, sinusitis, otitis media and septicemia. B)The non suppurative i-Acute rheumatic fever: Patients who had one attack of rheumatic fever have a significant risk of rheumatic heart. ii- Acute glomerulonephritis which follows even one attack of streptococcal infection . Dr. Asmaa 2009
Agent: Streptococcus pyogenes, beta Haemolytic streptococci group A .There are about 80 serological types . Dr. Asmaa 2009
Mode of transmission: • Contact : direct, indirect, droplets. • Air borne transmission. • Common vehicle ingestion of un-pasteurized milk. • Antibacterial immunity develops only against the specific strain that induced infection and may last for years. However, repeated attacks of sore throat due to different types of streptococci are frequent. • Passive natural immunity to streptococcus pyogenes occurs in newborns with transplacental transfer of maternal antibodies. Dr. Asmaa 2009
. Prevent streptococcal reinfection and possible recurrence of rheumatic fever : • Monthly injections of long acting penicillin. Patients allergic to penicillin can be given erythromycin orally. • Tonsillectomy: is indicted in • Chronic tonsillitis ( tonsillar hypertrophy that leads to obstructive sleep apnea) • Recurrent five attack a year for at least 2 years Dr. Asmaa 2009