Download

1 / 30
320 likes | 790 Views
AUTOIMMUNE DISEASES. Ass. Sklyannaya E.V. SYSTEMIC LUPUS ERYTHEMATOSUS . Systemic lupus erythematosus (SLE) is an autoimmune disease in which organs, tissues, and cells undergo damage mediated by tissue-binding autoantibodies and immune complexes. Epidemiology.

E N D
AUTOIMMUNE DISEASES Ass. Sklyannaya E.V.
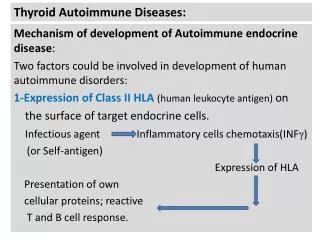
SYSTEMIC LUPUS ERYTHEMATOSUS Systemic lupus erythematosus (SLE) is an autoimmune disease in which organs, tissues, and cells undergo damage mediated by tissue-binding autoantibodies and immune complexes.
Epidemiology • Ninety percent of patients are women of child-bearing years. • Prevalence of SLE is 15 to 50 per 100,000.
Etiology environmental factors (estrogen, ultraviolet light) susceptibility genes abnormal immune responses
Pathogenesis • hypersensitivity of T and B lymphocytes • production of pathogenic autoantibodies • formation of immune complexes • sequestration and destruction of Ig-coated circulating cells • fixation and cleaving of complement proteins • release of chemotaxins, vasoactive peptides, and destructive enzymes into tissues
Pathology • In skin - deposition of Ig at the dermal-epidermal junction (DEJ), injury to basal keratinocytes, and inflammation dominated by T lymphocytes in the DEJ and around blood vessels and dermal appendages • In renal biopsies - proliferative changes in mesangium and in glomeruli, predominantly membranous changes to scarred glomeruli • In blood vessels - leukocytoclastic vasculitis • In lymph node biopsies - nonspecific diffuse chronic inflammation.
Clinical Manifestations • Systemic Manifestations (fatigue, myalgias, arthralgias,fever, prostration, weight loss) • Musculoskeletal Manifestations(polyarthritis, myositis) • Renal Manifestations (Nephritis) • Nervous System Manifestations(cognitive dysfunction, headaches, seizures, psychosis, myelopathy)
Clinical Manifestations Cutaneous Manifestations (lupus dermatitis: discoid lupus erythematosus, systemic rash, subacute cutaneous lupus erythematosus) The classic malar rash, also known as a butterfly rash, with distribution over the cheeks and nasal bridge. Note that the fixed erythema, sometimes with mild induration as seen here, characteristically spares the nasolabial folds. Photosensitive SLE rashes typically occur on the face or extremities, which are sun-exposed regions.
Clinical Manifestations • Vascular Occlusions • Pulmonary Manifestations • Cardiac Manifestations • Hematologic Manifestations • Gastrointestinal Manifestations • Ocular Manifestations
Workup • Tests for AutoantibodiesDiagnostically, the most important autoantibodies to detect are ANA since the test is positive in >95% of patients, usually at the onset of symptoms. High-titer IgG antibodies to double-stranded DNA (dsDNA) (but not to single-stranded DNA) are specific for SLE. • Standard Tests for DiagnosisScreening tests for complete blood count, platelet count, and urinalysis may detect abnormalities that contribute to the diagnosis and influence management decisions.
Diagnosis • 1. Malar rash. • 2. Discoid rash. • 3. Photosensitivity. • 4. Oral ulcers. • 5. Arthritis. • 6. Serositis. • 7. Renal disorder. • 8. Neurologic disorder. • 9. Hematologic disorder. • 10. Immunologic disorder. • 11. Antinuclear antibodies.
Differentials Antiphospholipid Syndrome, Fibromyalgia, Hepatitis C, Infectious Mononucleosis, Infective Endocarditis, Lyme Disease, B-Cell Lymphoma, Mixed Connective-Tissue Disease, Polyarteritis Nodosa, Preeclampsia (Toxemia of Pregnancy), Rheumatic Fever, Rheumatoid Arthritis, Scleroderma, Serum Sickness, Thrombotic Thrombocytopenic Purpura, Undifferentiated Connective-Tissue Disease, Drug-induced lupus erythematosus, Vasculitis, Leukemia, Neoplasia, HIV, Multiple sclerosis, Parvovirus or other viral infections.
Treatment • Analgesics • antimalarials • glucocorticoids • cytotoxic drugs
Prognosis Survival in patients with SLE is 90 to 95% at 2 years, 82 to 90% at 5 years, 71 to 80% at 10 years, and 63 to 75% at 20 years.
SYSTEMIC SCLEROSIS Systemic sclerosis (SSc) is a chronic multisystem disorder of unknown etiology characterized clinically by thickening of the skin caused by accumulation of connective tissue and by structural and functional abnormalities of visceral organs, including the gastrointestinal tract, lungs, heart, and kidneys.
Epidemiology The estimated incidence of systemic sclerosis is 19 cases per million population, and the prevalence of systemic sclerosis has been estimated at 240 cases per million population, although reported prevalence has ranged from 138 to 286 cases per million population. The risk of systemic sclerosis is 3-9 times higher in women than in men. The peak onset occurs in individuals aged 30-50 years.
Etiology • 1. Genetic abnormalities. • 2. Infectious agents. • 3. Environmental factors. • 4. Drugs.
Pathology • Systemic sclerosis is characterized by excessive fibrosis in the skin and other affected organs. The skin and lungs also show prominent T-lymphocyte infiltration. A severe fibroproliferative vasculopathy that affects small arteries and arterioles is universally present in affected organs. Platelet microthrombi are often found in the lumen of the narrowed vessels.
Classification 1. Systemic sclerosis: • Limited cutaneous disease • Diffuse cutaneous disease • Sine scleroderma • Undifferentiated connective tissue disease • Overlap syndromes 2. Localized scleroderma • Morphea • Linear scleroderma (en coup de sabre)
Clinical ManifestationsSkin Features • Tightening of the skin in the face, with a characteristic beaklike facies and paucity of wrinkles
Clinical ManifestationsSkin Features • Sclerodactyly with digital ulceration, loss of skin creases, joint contractures, and sparse hair
Clinical ManifestationsSkin Features • Anterior chest demonstrating salt-and-pepper hypopigmentation and diffuse hyperpigmentation in a white woman
Clinical Manifestations • Raynaud’s Phenomenon • Musculoskeletal Features • Gastrointestinal Features • Pulmonary Features • Cardiac Features • Renal Features
Workup • CT scan • Radiography • Echocardiography • Right-heart catheterization • Esophagraphy • Pulmonary function testing • Serum N-terminal pro-brain natriuretic peptide • Cardiac rhythm monitoring • Esophagogastroduodenoscopy • Biopsy of skin and lungs
Diagnosis Preliminary criteria of systemic sclerosis by the American Rheumatism Association: major criterion sclerodermatous involvement proximal to the digits minor criteria: 1)sclerodactyly, 2)digital pitting scars or tissue loss of the volar pads of the fingertips, and 3)bibasilar pulmonary fibrosis.
Differentials • Eosinophilia, Eosinophilia-Myalgia Syndrome, Eosinophilic Fasciitis, Graft Versus Host Disease, Mycosis Fungoides, Primary Biliary Cirrhosis, Pulmonary Hypertension, Primary, Reflex Sympathetic Dystrophy, Scleroderma. Other Problems to be Considered:Toxic oil syndrome (adulterated rape seed oil), Porphyria cutanea tarda, Digital sclerosis of diabetes mellitus, Vibration disease, Radiation exposure, Intestinal obstruction, Infiltrative cardiomyopathy, Nephrogenic fibrosing dermopathy (nephrogenic systemic fibrosis), Amyloidosis, Scleromyxedema (generalized lichen myxedematosus), Scleredema diabeticorum
Treatment • D-penicillamine, • colchicine, • IFN-γ, • IFN-α, • recombinant human relaxin, • antiplatelet therapy, • glucocorticoids, • calcium channel blockers
Prognosis • Pulmonary hypertension and scleroderma renal crisis are the most frequent causes of mortality. Survival averages 12 years from diagnosis and correlates best with the clinical disease subtype (diffuse cutaneous vs limited cutaneous) and extent of organ involvement. • The limited cutaneous subset carries a 10-year survival rate of 71%. The diffuse cutaneous subset carries a 10-year survival rate of 21%. Pulmonary hypertension is a major prognostic factor for survival.