Download
1 / 45
480 likes | 1.02k Views
Detecting Antibodies. The Antibody Screen. CLS 422 Clinical Immunohematology I. Objectives. Explain the purpose of performing an antibody screen. Discuss the antigen characteristics important in the composition of screening cells. Describe the phases of antibody detection.

E N D
Detecting Antibodies The Antibody Screen CLS 422 Clinical Immunohematology I
Objectives • Explain the purpose of performing an antibody screen. • Discuss the antigen characteristics important in the composition of screening cells. • Describe the phases of antibody detection. • Describe the types of antibodies that can be encountered in each of the phases of antibody detection.
Objectives • State the difference between an alloantibody and an autoantibody. • List factors affecting the antigen-antibody reaction in the indirect antiglobulin test. • Discuss the action of potentiators. • Compare and contrast methods for performing an antibody screen. • Assess sources of error affecting the indirect antiglobulin test. • Interpret the results of an antibody screen.
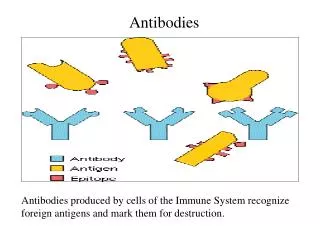
The Antibody Screen • Used to detect “irregular” antibodies. • Maximize detection of clinically significant antibodies • Minimize detection of insignificant antibodies • Patient’s serum or plasma is tested against reagent red blood cells (RBCs) with known antigens (screen cells).
Allo vs. Auto • Alloantibody – antibody directed against antigens that the individual does not possess • Immune • Naturally-occurring • Autoantibody – antibody directed against one’s own antigens • Auto control – patient’s RBCs tested against patient’s plasma
What makes an antibody clinically significant? • The ability to cause decreased RBC survival. • If the antibody activates complement, there may be intravascular RBC lysis. • There may be extravascular destruction of antibody-coated RBCs by the macrophages of the RES. • Hemolytic Transfusion Reaction (HTR) • Hemolytic Disease of the Fetus & Newborn (HDFN)
Who needs to be tested? • OB patients – looking for antibodies that may cause HDFN in the fetus. • Patients who need an RBC transfusion – looking for antibodies in the recipient that could destroy the donor RBCs (HTR). • Blood, organ and tissue donors – avoid passive antibody transfer; evaluate as source of anti-serum and rare RBCs.
An Application of the Indirect Antiglobulin Test • Patient’s plasma (unknown antibody) is tested against reagent RBCs (known antigen). Y Y Y • Incubated at 37oC to allow antibody to sensitize RBCs. • Antiglobulin phase to allow sensitized RBCs to agglutinate.
Screen Cell Composition • Sets of 2 to 4 different cells • Group O • Rh Positive and Rh Negative cells • Other major blood group antigens are represented
Antigen Profile (Antigram) • If the patient’s serum/plasma contains an antibody directed against one of the antigens on the screen cell, the RBCs will agglutinate (or hemolyze)= positive reaction. • We can not be certain which antigen is the target of the antibody.
Immediate spin (I.S.) (optional phase) 37oC AHG Lewis, M, N, P1, cold autoantibodies (I, H, IH) May see D, E, K, strong cold antibodies Rh, Kell, Kidd, Duffy, Ss Phases of Testing
Specimen • Plasma • Serum
Antibody Screen Tube Method ID I 37C inc ID II ID III √ √ √
Ortho Provue Courtesy Ortho-Clinical Diagnostics Raritan, NJ
Antibody Screen Solid Phase Adherence Method • RBC antigens are bound to the sides of a microtiter well. • Different wells possess different antigens, and thus are different “screen cells”.
Immucor Automation • ABO and Rh are performed using direct agglutination in a microtiter well. • Screens, panels and DATs are performed using solid phase adherence.
Reporting Results • Reporting is “all or nothing”, rather than reporting the results of each cell at each phase. • If all cells are nonreactive at all phases, and the Coombs Control Cells are positive, the screen is reported as negative.
Reporting Results • If one or more cells react at any phase of testing, the screen is reported as positive. • An antibody panel should be performed to determine the specificity of the antibody present.
Are We Done Now? • NO – all cells should be tested through all phases, even if a positive reaction has already been observed.
How Would you Report This Screen?(Performed Using Solid Phase Adherence)
Factors Affecting the Antibody Screen These factors will affect ANY application of the indirect antiglobulin test!
Antigen/Antibody Ratio Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Postzone Prozone Equivalence Ratio is usually 2 drops of serum or plasma to 1 drop of RBC suspension.
Reaction Time • IgG antibodies are incomplete • Require incubation at 37oC to react • Length of incubation dependant on test medium
Test Medium • May add potentiators to overcome the effects of shielding and the zeta potential • Albumin • LISS • PEG • Enzymes
pH • Optimal 6.5 to 7.5
Sources of Error in the Antibody Screen False Negative Results
Improper Wash Y Y Y Y Y Y Y Y Y Y Y Y
Failure to… • Add plasma (the antibody source) • Make it a habit to add plasma to tube before adding RBCs. • Add reagents • Follow manufacturer’s directions • Recognize hemolysis as a positive reaction
Work Quickly Y Y Y Y Y Y Y
Other causes of false negative results • AHG reagent neutralized • Using expired reagents • Under-centrifugation • Complement-dependant antibody/plasma specimen
Sources of Error in the Antibody Screen False Positive Results
False Positives • Over-centrifugation • Contaminated reagents • Debris • Rouleaux
Limitations of the Antibody Screen • Will not detect ABO incompatibility • Will not detect antibodies to antigens that are not present on the screen cells • May not detect antibodies exhibiting dosage • May not detect antibodies that are low in titer
Primary vs. Secondary Humoral Response IgG IgM IgM IgG First exposure Second exposure