Download
1 / 25
260 likes | 565 Views
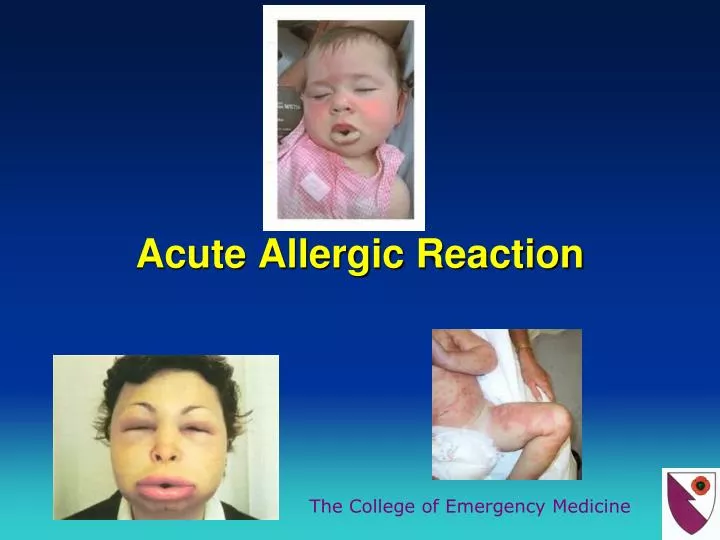
Acute Allergic Reaction. Acute Allergic reaction. Ranges from rash to fatal anaphylaxis. Allergies are among the most common diseases in the UK Around 30% of adults and 40% of children are affected. Anaphylaxis.

E N D
Acute Allergic reaction Ranges from rash to fatal anaphylaxis
Allergies are among the most common diseases in the UK Around 30% of adults and 40% of children are affected
Anaphylaxis Anaphylaxis is a severe, life threatening, generalised or systemic hypersensitivity reaction characterised by rapidly developing life threatening problems involving airway, breathing and circulatory problems with associated skin and mucosal changes.
UK Incidence • No overall figure is available in the UK. • 500,000 venom induced anaphylactic reaction reported • 220,000 had nut induced allergic reaction in under the age of 44 years old reported. • 1 in 1333 people have experienced an anaphylaxis reaction in their life time.
The overall mortality of anaphylaxis • has been estimated at <1%. • Over half of all deaths due to anaphylaxis occur • within an hour of allergen exposure. • Primarily from asphyxia due to upper airway • oedema and bronchospasm, or hypotension and circulatory failure.
Anaphylaxis is caused by the degranulation of mast cells and basophilswithsubsequent release of inflammatory mediators such as histamine, tryptase, prostaglandins, leukotrienes, cytokines and chemokines. These inflammatory mediators cause smooth muscle contraction, vasodilation and increased vascular permeability, leading to urticaria, angioedema, bronchoconstriction and hypotension.
People presenting with mild to moderate allergic reactions can later develop anaphylaxis particularly it is more common in high risk group. eg: Asthmatics and people with known anaphylactic reactions to food and venoms.
The most common signs and symptoms of anaphylaxis are cutaneous (generalised urticaria, angioedema, flushing and itching), affecting around 90% of patients. Other features include respiratory symptoms (dyspnoea, wheeze, stridor or hypoxia), affecting70%, and GI symptoms such as abdominal pain and vomiting, affecting 40%. Hypotension is less common, affecting between 10−30% of patients with anaphylaxis.
Pathophysiology • Immunologic mediated (IgE mediated foods, insects, drugs and latex) • Non-immunologic mediated (most drugs) • Idiopathic
Reactions can be triggered by virtually any agent capable of activating mast cells and basophils, but the most commonly implicated allergens are; • Foods (particularly milk, egg, peanuts, tree nuts, fish, shellfish, soy and wheat) • Drugs • Stings or venoms • Latex • Allergen immunotherapy injections
Food is common in children • Drugs are more common in adults
Stings 47; 29 wasp, 4 bee, 14 unknown • Nuts 32; 10 peanut, 6 walnut, 2 almond, 2 brazil, 1 hazel, • 11 mixed or unknown • Food 13; 5 milk, 2 fish, 2 chickpea, 2 crustacean, 1 banana, • 1 snail • Food possible cause 17; 5 during meal, 3 milk, 3 nut, 1 each - fish, yeast, • sherbet, nectarine, grape, strawberry • Antibiotics 27; 11 penicillin, 12 cephalosporin, 2 amphotericin, • 1 ciprofloxacin, 1 vancomycin • Anaesthetic drugs 39; 19 suxamethonium, 7 vecuronium, 6 atracurium, • 7 at induction • Other drugs 24; 6 NSAID, 3 ACEI, 5 gelatins, 2 protamine, • 2 vitamin K, 1 each - etoposide, acetazolamide, • pethidine, local anaesthetic, diamorphine, • streptokinase • Contrast media 11; 9 iodinated, 1 technetium, 1 fluorescein • Other 3 1 latex, 1 hair dye, 1 hydatid
The diagnosis is suspected clinically on the basis of the patient's symptoms and confirmed biochemically
Always record the time of onset of symptoms. • Clinical and biochemical diagnosis • Mast cell tryptase should be done immediately and 1-2 hours after the treatment not more than 4 hours.
All children under 16 should be admitted • All adults who have had emergency treatment should be observed for 6-12 hours after the onset of symptoms because of the risk of bi-phasic reaction.
Discharge patients after an anaphylactic reaction with specialist referral and auto-adrenaline injector (epi pen)
Biphasic anaphylaxis • After complete recovery of anaphylaxis, a recurrence of symptoms within 72 hours with no further exposure to the allergen. It is managed in the same way as anaphylaxis