Download
1 / 28
390 likes | 1.04k Views
Snapping Scapula Syndrome. Robert Whittaker, SPT University of North Dakota. Overview. First described in 1867 by Boinet 1 Mauclair later described 3 subclasses Froissement – physiologic friction sound

E N D
Snapping Scapula Syndrome Robert Whittaker, SPT University of North Dakota
Overview • First described in 1867 by Boinet1 • Mauclair later described 3 subclasses • Froissement– physiologic friction sound • Frotting – louder grating sound associated with pathologic alterations (soft tissue problems) • Craquement– pathologic loud snapping sound (loud/painful grating sounds by osseous anomalies) • http://youtu.be/CTbQG7Jp3Zw • Snapping Scapula (or washboard syndrome1) – painful crepitus of scapulothoracic (ST) articulation, commonly seen in overhead-throwing athletes (noises amplified by thoracic cavity such as a resonance chamber of stringed instrument)2 • Dyskinesias caused by pain & muscle weakness, imbalances, inflexibility
Overview Continued • Dyskinesia can increase anterior tilt, decrease scapular upward rotation, and increase scapular internal rotation1 • Anteriorly tilted scapula compresses medial border against ribs and scapula pivots around its medial border rather than sliding laterally • Practice Pattern 4E: Impaired Joint mobility, Motor Function, Muscle Performance, and ROM Associated With Localized Inflammation6 • ICD-9-CM Code: 727.3 Other Bursitis • Prognosis: Over the course of 2-4 months pt. will demonstrate optimal recovery (6-24 visits)
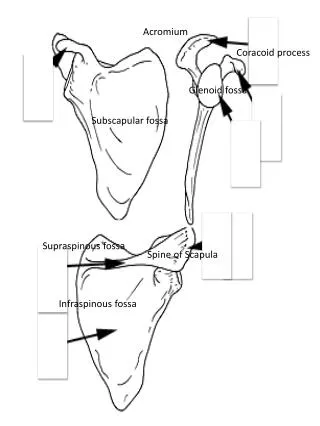
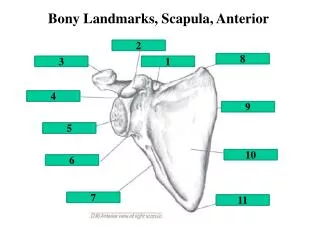
Anatomy • Scapula’s Role – maintain stable BOS for humerus and dynamic positioning of the glenoid during GH elevation.2 • Clavicle acts as strut for scapula opposing medially directed forces of axioscapular muscles and allowing scapular rotation and translation along thoracic cage • Muscle tendons and bursa located between thorax and scapula – several bursa around ST joint to facilitate smooth movement have potential for scapular dysfunction/crepitus • Supraserratus (subscapularis) bursa – between subscapularis, serratus anterior, & axilla1 • Infraserratus (ST) bursa – between serratus anterior, chest wall, & rhomboids1 (facilitates gliding of serratus on chest wall3) • Adventitial bursa (inconsistent findings)2 • Superomedial angle: 1 infraserratus & 1 supraserratus • Inferomedial Angle: 1 infraserratus • Trapezoid bursa located at base of spine of scapula
Neurovascular Anatomy3 • Spinal Accessory N • Goes through levator scapula close to superomedial angle & runs along medial border deep to trapezius muscle • Traverse cervical A • Branches anastomose into dorsal scapular A & suprascapular A (superficial branch flows with accessory N) • At risk with portal placement cranial to scapular spine or with inadvertent dissection during open approach3 • Suprascaupar N & A run toward suprascapular notch • At risk if superomedial scapular resection or superior arthroscopic portal3 • Dorsal scapular A flows with dorsal scapular N 1cm medial to medial border • Dorsal scapular N/A provides innervation to rhomboids & deep to them • Long thoracic nerve located on surface of serratus anterior • Infrequently at risk3
Pathology • Crepitus caused by irritation of several bursa around the scapula2 • Chronic, forceful repetitive actions of shoulder mechanisms can induce micro-tears along periosteum at the medial border of the scapula causing a traction osteophyte at muscular attachment of scapula.2 • Osseous lesion (i.e. osteochondroma) in ST space may become pathologic • Muscle atrophy (disuse/nerve injury) leads to diminished soft tissue interposition between thorax and scapula • Anatomical variance can lead to incongruity – superomedial & inferomedial angles can have hook shape, Lushkatuberkle • Scoliosis & thoracic kyphosis • Healing fractures of rib/scapula with bony angulation • May not always be pathologic, snapping may lead to painful symptoms over time
Diagnosis2 • Complaints of pain with increasing activity • Scapular noise/crepitus with motion of scapula (single to multiple noises or only palpation) • Tenderness at superior angle & medial border of scapula • Pain over levator scapula, trapezius, & or rhomboids due to contracture & malfunction1 • History of overuse (sports including swimming, pitching, weight training, gymnastics, and football) • Observation of (B) asymmetry in scapula • Handedness may result in slight depression • Winging commonly noted • Moderate to severe forward head and anterior rounded shoulders
Diagnosis2 • Assess • Flexibility & soft tissue tightness in surrounding muscles (tight Pec Minor contribute to faulty scapular mechanics) • Muscle length & strength (upper/lower trapezius, rhomboids, serratus anterior, latissimusdorsi, levator scapula, rotator cuff, & deltoid. • Scapulohumeral Rhythm (GH elevation:ST rotation 2:1) • Elevation induces posterior tilting and scapular ER • Faulty patterns include decreased GH motion with increased scapular motion during elevation • Pain normally not reproducible with isometrics1 • Crepitus easily reproduced with arm movements, pain reproduced generally with shoulder abd1 • May be accentuated with compression of superior angle against chest wall • Pain & snapping decrease with crossing the arm lifting scapula from ribcage1 • Pseudowinging may be present to compensate for pain with motion
Diagnosis1 • Imaging • AP & tangential view • 3D CT to visualize congruity • Fluoroscopy to visualize grating/snapping during shoulder motion • MRI for soft tissue lesion • Selective injections of local anesthetic/steroid for symptomatic bursa – transient relief, inflammation likely present3
Differential Diagnosis2 • Cervical spine radicular symptoms (Spurling test for radicular symptoms) • C5-C8 can cause symptoms of scapular pain • Quick manual cervical myotome test can help rule out nerve origin pain • GH Joint referred pain • Shoulder impingement can alter normal scapulohumeral rhythm, compensates by elevating or protracting scapula to elevate arm more. Leads to overuse of scapular muscles • Electromyogram & nerve conduction time to determine if scapular winging is neurological injury • Other Noises? • Trigger point referrals: multifidi, trapezius, levator scapula, scalenes, serratus posterior superior, serratus anterior, latissimusdorsi, & rhomboids
Conservative Management2 • Pain releivingmodalities (diathermy, ultrasound, and iontophoresis to undersurface of medial border) • Local injections and NSAIDs (If pain persists, PT must be avoided & injections considered1) • Strengthening of weak muscles • Rhomboids, mid/lower trapezius, serratusanterior, teres minor, infraspinatus, posterior deltoid, &longuscolli/capitis (most common lower stabilizers, serratus anterior, mid/lower trapezius) • Serratus anterior weakness can cause forward tilting inducing crepitus1 • Focus on subscapularis & serratus anterior if atrophied3 • Scapular add & shoulder shrug strengthen scapular stabilizers (serratus anterior, rhomboids, levator scapular)1 • Abduction & elevation of scapula should be avoid from increased pressure and strain on underlying musculature1 • Strengthening inhibited/functionally weakened muscles in both OKC & CKC
Continued conservative2 • Endurance training should be emphasized due to primary function of scapula of static posturing of shoulder girdle • Muscle fatigue can lead to compensatory motion • Many roles of scapula are eccentric • Patterns of movement that include pt’s. required activities • CKC advantageous in early stages because of stabilization effects • Progression from isometric & isotonic to endurance eccentric strengthening • Scaption, press-up, rowing, push-up+ • Advanced: eccentric scapular control (plyometric exercises such as plyoback, D2 PNF, Swiss ball isometric holds
Conservative Management2 • Stretching of tight muscles • Pectoralis major/minor, levator scapula, upper trapezius, latissimusdorsi, subscapularis, SCM, rectus capitis, & scalenes • Weak muscles cannot be optimally strengthened if antagonists not stretched • Postural correction • Thoracic kyphosis, forward head, rounded shoulders, abducted and anterior tilted scapula, sub occipital extension • Will allow for maximal neuromuscular efficiency and improved biomechanics • Reduce kyphosis will improve congruency3 • Use of thoracic spine mobilization to promote correction • Core strengthening – crossroads for energy from LE<->UE
Conservative Management2 • Lower scapular stabilization can be facilitated with contraction of contralateral gluteus maximus via thoracolumbar fascia • Pain & inflammation should be guide throughout progression • 3-6 months conservative treatment failure, surgical options may be considered • Pts. likely to fail include nerve deficits due to damage, bony incongruities, and those who can snap their scapulas & do so frequently out of habit • Crepitus related to soft tissue, altered posture, winging, or dyskenisa surgery may not be required1
Operative Management2 • Pts. with cervical spine & neurological impairment excluded • Failure to have pain relief after preoperative injection may be contraindicated • Open surgical resection of superomedial angle of scapula (most common for bone incongruity) • Supraspinatus, rhomboid, and levator scapula are dissected free & superomedial angle resected with oscillating saw & smoothed with rongeurs. • Sling & PROM begins immediately, AROM added at 8 weeks, resistance at 12 weeks
Operative Management2 • Bursectomy rather than superomedial angle resection as bone histologically and grossly normal even despite good results • Open procedure • Inferior angle (infraserratus1) • Oblique excision distal to inferior angle. Trapezius & latissimusdorsi split in line with their fibers exposing bursa • Bursa sharply excised & any osteophytes removed • PT at week 1, gentle throwing in athletes at week 6 • Superomedial Bursa2 • Vertical incision made medial to vertebral border, trapezius dissected free (accessory nerve protect1), subperiosteal dissection to free levator scapula & rhomboid and preserve tendinous attachments (dorsal scapular 2cm from medial border protect1) • Bursa resected & bony abnormalities removed, muscles reapproximated with bone drill holes and wound closed in layers with absorbable sutures • Sling for comfort, PROM & pendulum exercises immediately, AROM at week 3, strengthening at week 6, gentle throwing at week 12
Superomedial Open Resection3 • Immobilized up to 4 weeks in sling • Pendulum & PROM exercises immediately • AROM ~8 weeks • Strengthening ~12 weeks to periscapularmuscles
Operative - Arthroscopic2 • Low invasiveness, decrease morbidity & preservation of muscle attachments, early postop rehab, shorter hospital stay, & higher compliance1 • Painful trapezoid bursa may be missed with arthroscopy • Access & visualization of superior angle of scapula with standard portals (inferior to scapular spine 3-4 fingerbreadths from medial scapular border to avoid dorsal scapular nerve & artery, accessory nerve, & neurovascular structures at superomedial angle of scapula) • After portal positioning, arm brought into chicken wing position to proceed with arthroscopy
Operative – Arthroscopic1 • Pt. prone/lateral position with arm IR “chicken wing” • 2 medial portals to view at level of scapular spine, second is working portal located inferior to spine • Upper portal 3cm medial to spine of scapula through skin to pass trapezius, plane between rhomboid major & minor, serratus anterior (caution to avoid pneumothorax or perforate serratus anterior) • Inferior portal between scapular spine & inferomedial scapular angle (instruments point away from coracoid process to reduce suprascapular N injury when working in subscapularis space) • 3rd superior portal useful when ST bursectomy associated with resection of superomedial angel of scapula
Operative – Arthroscopic1 • 3rd Portal – Using superomedial angle of scapula & lateral border of acromion as landmarks, the position is located between the middle & medial thirds of the line joining these 2 points (anatomical sites of entry must be respected to avoid damage to neurovascular structures & trocar must be passed through as close to ventral surface of scapula as possible to avoid penetration of the thoracic cavity • Inside-out method starting with arthroscope in viewing portal that is directed superiorly from ST space just laterally to the point marked with a needle and exit in the previously marked region corresponding to superior portal • Arthroscopeintroduced in viewing portal using fluid pressure of 50-60mmHg to ST space • Inferior working portal or from superior 3rd portal instruments are introduced to carry out the procedure (bleeding controlled with radiofrequency device) • Fibrous tissues removed with shawerto find subscapularis (supraserratus) bursa • Supraserratus & infraserrtausbursa & any fibrous adhesions around removed to expose superomedial angle – resection of superomedialangle if there is a prominence • Careful to avoid suprascapular N damage by directing shawer from superior portal to skin target equidistance from spine to inferior angle.
Operative – Arthroscopic1 • Rehab • Passive mobilization 1st post op day • Full AROM within 1-2 weeks • Strengthening should be allowed after 30 days • Pt. return to sport 3rd postop month • Other3 • Sling for comfort and discontinued within 1 week • Pendulum & PROM exercises immediately • AROM & Strengthening Based on tolerance
Conclusion2 • Good to excellent results • Most return to work/sport within 3-4 months regardless of operation • Important to address proper thoracic posture, scapular control, and strength before return to activity
References • MerollaG, Cerciello S, Paladini P, Porcellini G. Snapping scapula syndrome: Current concepts review in conservative and surgical treatment. Muscles Ligaments Tendons J. 2013;3(2):80-90. doi: 10.11138/mltj/2013.3.2.080; 10.11138/mltj/2013.3.2.080. • ManskeRC, Reiman MP, Stovak ML. Nonoperative and operative management of snapping scapula. Am J Sports Med. 2004;32(6):1554-1565. doi: 10.1177/0363546504268790. • GaskillT, Millett PJ. Snapping scapula syndrome: Diagnosis and management. J Am AcadOrthop Surg. 2013;21(4):214-224. doi: 10.5435/JAAOS-21-04-214; 10.5435/JAAOS-21-04-214. • Goodman CC, Fuller KS. Pathology: Implications for the physical therapist. SAUNDERS W B Company; 2009. • KisnerC, Colby LA. Therapeutic exercise: Foundations and techniques. F a Davis Company; 2007. • Guide to physical therapy practice. 2nd ed. APTA; 2003.