Download
1 / 44
440 likes | 583 Views
Genetic and Environmental Influences Underlying Depression. Maya Subbarao EHS 504 3-23-2005. What do these people have in common?.

E N D
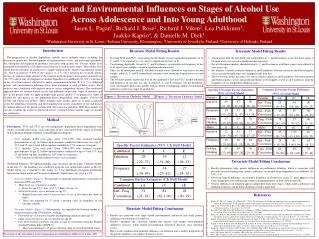
Genetic and Environmental Influences Underlying Depression Maya Subbarao EHS 504 3-23-2005
What do these people have in common? Princess Diana, Mike Wallace, Tipper Gore, Winston Churchill, Barbara Bush, Sir Isaac Newton, Winona Ryder, Bonnie Raitt, Drew Cary, Jim Carrey, Paul Simon, Abraham Lincoln, Richard Dreyfuss, Oksana Baiul, Monica Seles, Ralph Nader, Jackson Pollack, Judy Collins, Larry King…
Presentation Overview • What is Depression • Monoamine Hypothesis • The Role of Serotonin • Underlying Genetics • Caspi et al. (2003) and Kaufman et al. (2004) • Genetic Testing Considerations
What is Depression? • Diagnostic and Statistical Manual of Mental Disorders-4th Edition. (American Psychiatric Association, 1994) • Allows clinicians to communicate and conceptualize a disorder with a wide array of symptoms • Allows for agreement on symptoms that define a disorder • Educational tool and reference in conducting clinical trials, prevalence studies, and outcome research • Not used to categorize and/or label individuals—Remember a person has cancer, but is not cancer themselves.
What is Depression? • Among the top 5 leading causes of disability and disease burden throughout the world (Tang and Lopez, 1997) • Stressful events involving threat, loss, humiliation influence onset and course of condition. • Diagnoses can be made on affective, behavioral, cognitive, somatic symptoms • Affective—depressed mood, feeling of worthlessness, guilt • Behavioral—social withdrawal, agitation • Cognitive—difficulty in concentration or making decisions • Somatic—insomnia, hypersomnia
What is Depression? • Focus on Major Depressive Disorder (MDD) • Melancholic Features: at least three of the following: loss in pleasure in most activities, depressed in morning and wake up agitated, extreme feelings of guilt, substantial weight loss, affects men and women equally but more prevalent among the elderly, treated with antidepressants. • Atypical Features: brightened mood when good things happen, at least two of the following: substantial weight gain, sleeping too much, sensitivity to rejection, more commonly seen in teens, women are 2-3 times more likely to be affected. • SAD—symptoms begin in fall and end in spring, seen with recurrent MDD
Genetics of Depression—What we know • Complex mode of inheritance—multiple genes that interact with each other & environment? • Different susceptibility genes in different families • Parameters of penetrance of the variant allele and its frequency are unknown • First degree relatives have 3 fold increase in chance of developing MDD. • Heritability of 40-70% • Genetic factors may be shared with generalized anxiety disorders
Molecular Genetics of Depression • Zubenko et al. (2003) found several loci that may underlie MDD—81 family study • Concluded that “Gene products derived from…genes that participate in cellular signaling pathways that converge on CREB and that allelic variants of the downstream target genes of CREB may affect the susceptibility of mood disorders.” • Abkevich et al. (2003) investigated 1890 individuals from 110 pedigrees and discovered that 12q22-12q23.2 is a sex-specific disposition locus for MDD.
Monoamine Hypothesis of Depression • “The underlying biological or neuroanatomical basis for depression is a deficiency of central noradrenergic and/or serotonergic systems and that targeting this neuronal lesion with an antidepressant would tend to restore normal function in depressed patients” (Hirschfeld, 2000). • Formulated over 30 years ago based on the mechanisms of antidepressants
Formulation of the Monoamine Hypothesis • 1950’s research on lysergic acid diethlamide (LSD) showed that this hallucinogen blocked peripheral serotonin receptors. • Reserpine (antihypertensive agent) depleted brain serotonin and increased 5-HIAA in urine, thus inducing depressive symptoms in individuals. • In 1951, isoniazid and iproniazid found to inhibit MAO, which degrade serotonin and norepinephrine in tubecular patients. • By early 1960’s, use of tricyclic antidepressants (TCAs) as reuptake inhibitors—drastic side-effects • Development of Selective Serotonin Reuptake Inhibitors (SSRIs) • Although there are limitations to the hypothesis, it has been basis for current research on the biological basis of depression.
Evidence of Serotonin’s Role in the Monoamine Hypothesis • Increase in density of postsynaptic 5-HT2 receptor binding sites in frontal cortices of un-medicated depressed patients (Stanley and Mann 1983). • 5-HIAA levels lower than normal in CSF of depressed patients (Lowther et al., 1997). • Number of transporter sites reduced in platelets of antidepressant-naïve depressed patients, but no alteration of transporter sites in people with atypical depression. • Gibbons and Davis (1984) show that concentration of serotonin is reduced in hypothalamus and amygdala of postmortem brain tissue in patients with depression.
Evidence for the Role of Serotonin • Studies conducted in which a tryptophan-free drink was administered to patients • 67% of patients who were responding to antidepressants two weeks prior to investigation, had relapse in depressive symptoms within 5-7 hours of trp depletion (Delgado 2000) • Lack of depressive symptoms upon trp depletion in un-medicated depressed individuals and in healthy individuals—dysfunction not at level of neurotransmitter. • Benkelfat et al. (1994) showed that 30% of subjects who had a family history demonstrated depressive symptoms upon trp depletion.
Genetics of Depression—Serotonin (5-HT) • 5-HT transport protein (5-HTT) is involved in regulation of serotonin • 5-HTT expression mainly in cortical and limbic areas of brain associated with behavior and emotions • 5-HTT encoded by SLC6A4 gene located on chromosome 17q12
Serotonin and Depression • Gene-linked polymorphic region called 5-HTTLPR, which is located 5’ to the SLC6A4 gene. • 5-HTTLPR site is composed of 16 repeat elements. The polymorphism results in either a 44bp insertion or deletion. • Short (s) and long (l) • Lesch et al. (1996) transfected lymphoblastoid cells with luciferase reporter and fused this to the 5-HTTLPR region. • Discovered that the l variant had twice as much basal txn than s variant. • l/l were 30-40% more likely to bind [125I]RTI-55 and 1.9-2.2 times more likely to take up [3H]5-HT
Lesch et al. (1996) Association of Anxiety-Related Traits with a Polymorphism in the Serotonin Transporter Gene Regulatory Region. Sicen Science274: 1527-31.
Influence of Life Stress on Depression: Moderation by a Polymorphism in the 5-HTT Gene Caspi, A., Sugden, K., Moffitt, T.E., Taylor, A., Craig, I.W., Harrington, H., McClay, J., Mill, J., Martin, J., Braithwaite, A., and Poulton, R. Science (2003) 301: 386-89.
Caspi et al.’s Investigative Approach • 5-HTT may “moderate the serotonergic response to stress” even though it may not be directly associated with depression. • Three lines of evidence for a GXE interaction: 1) -/- and +/- mice exhibited greater fear and elevated adrenocorticotropin when responding to stress 2) -/- and +/- in Rhesus macaques correlated with decrease in 5-HIAA in CSF in monkeys raised in stressful environments compared to those raised in non-stressful environments. 3) s/s and s/l had greater amygdala neuronal activity when exposed to scary pictures (Hariri et al., 2002).
Neuronal Amygdala Imaging in Response to Fearful Stimuli Hariri et al. (2002) Serotonin Transporter Genetic Variantion and the Response of the Human Amygdala. Science297: 400-403.
The Fearful Stimuli Hariri et al. (2002) Serotonin Transporter Genetic Variantion and the Response of the Human Amygdala. Science297: 400-403.
Study Design • 847 Caucasian, no-Maori from Dunedin Multidisciplinary Health and Development Study • Used life-history calendar to assess stressful events between 21st-26th birthday • Stressful events included: relationship stressors, education, employment, housing, finances • 5-HTTLPR genotype did not influence exposure to stressful events since no significant difference in number of events experienced between groups • Diagnosed using DSM-IV criteria and Diagnositc Interview Schedule • “Tested association between depression and 1)5-HTTLPR genotype 2) stressful life events 3) their interaction”
Caspi et al.’s Results • By age 26, self-reports of depression were higher for s/s and s/l individuals (p<0.02) • Carrying s allele predicted MDD diagnosis in individuals who did not have prior history of depression (p=0.002 for s/s and p=0.001 for s/l) • Similar findings for suicide ideation and self-reports of depression
Caspi et al.’s Results Continued… • Lack of evidence for GXG interaction (ie: individuals have genetic susceptibility to enter stressful events) • If stressful events represented influential environmental factors, then depression should not be predicted prior to 21st birthday since life-events were not assessed at this point
5-HTT and Childhood Maltreatment • Interaction between 5-HTTLPR and maltreatment predicted adulthood depression only among s allele carriers • P=0.05
Limitations of Study • Unable to test endophenotypes since it is difficult to take CSF • Environmental exposures hard to control and gene effects may be conditional on these exposures • Further studies needed to confirm results
Social Supports and Serotonin Transporter Gene Moderate Depression in Maltreated Children Kaufman, J., Yang, B.Z., Douglas-Palumberi, H., Houshyar, S., Lipschitz, D., Krystal, J.H., Gelernter, J. PNAS 2004 101: 17316-17321
Depression one of the most common sequelae reported in maltreated children. • Caspi et al. (2003) focus only on adults with current life-stressors • Studies have shown that non-human primates raised in stressful situations (peer-reared) with s allele show increased emotional distress, elevated HPA response to stress, and basal serotonergic function (Barr et al., 2003). • Purpose: Identify if the provision of social supports modifies the development of depression in maltreated children.
Results • Maltreated children had significantly higher depression scores compared to CC’s. • l/s and l/l maltreated children only had slightly higher depression scores than CC’s of the same genotype. • s/s maltreated children had depression scores twice as high as both CC’s and other maltreated children. • s/s maltreated children with low social supports had depression scores twice as high as CC’s of same genotype and social situation.
Contact with Primary Support • Who the child talks to problems about, buys items of need, spends time with/has fun • 20% maltreated children report seeing primary support less than a few times per year • Maltreated children with at least one s allele and with minimal contact with the primary support showed a 33% increase in depression score
Is depression gendered? • Caspi et al.’s (2003) study is hard to replicate because different populations are exposed to different stressors at varying frequencies. • Women are twice as likely to suffer form an MDD episode than men. (Kessler et al., 1994) • Eley et al. (2004) showed that there is an increased risk for depression in adolescent females with the s/s genotype and exposed to high environmental risk, but not for males. • Grabe et al. (2005) Study of Health in Pomerania (SHIP) showed that s-allele increased depression scores for females, but not males, who had low social support and were facing unemployment (with genotype—22.8% variation in BL-38 score, without genotype—20.9%)
Overarching Conclusions • s-allele confers a vulnerability to depression in individuals with life history of stress • Under non-stressful conditions, s allele does not increase/decrease risk for depression • Negative sequelae associated with stress during early development • Social support may be used to promote resiliency.
Drug Therapies for Depression • Selective Serotonin Reuptake Inhibitors: -Fluoxetine (Prozac) -Paroxetine (Aropax) -Citalopram (Cipramil) -Fluvoxamine Sertraline (Zoloft) • Prevents reuptake of 5-HT at the nerve synapses • Takes 2-6 weeks to see anti-depressant effects—which is a reason for non-compliance.
SSRI’s and Depression • If the s-allele of 5-HTTLPR reduces txn of the transporter, how can SSRI’s have a therapeutic effect? • Smeraldi et al. (1998) showed that l/l and l/s individuals had better response to fluvoxamine alone than s/s individuals • Fluvoxamine and pindolol improved outcomes for all genotypes
Why is that? • Hypothesize that SSRI’s stimulate increase in 5-HT at the raphe nuclei—activates somatodendritic 5-HT1A autoreceptors—negative feedback. • 5-HTT mRNA abundant in dorsal raphe nucleus, the initial site of the negative feedback “as its 5-HT neurons project into the frontal cortex and are very sensitive to self inhibition by 5-HT1A autoreceptors” • In s/s individuals the same SSRI dose leads to hyper negative feedback. • Pindolol is 5-HT1A antagonist and prevents negative feedback
Genetic Screening for susceptibility to depression: can we and should we? • Morley, Hall, Carter (2004) Australian and New Zealand Journal of Psychiatry38: 73-80. • DSM-IV broad definitions mean that people can develop the disorder through different “pathological pathways with different genetic contributions.” • Problems of genetic heterogeneity, gene-gene interaction, cultural differences in expression
Genetic Testing? • We do not have preventative pharmacological treatments—problems of cross-talk • Genetic testing can disrupt family dynamics, particularly for minors. Parents may lower their expectations for their child and alter how they relate to the child (Cohen 1998). Stigmatization and discrimination?
Works Consulted • Abkevich, V., Camp, N.J., Hensel, C.H., Neff, C.D., Russell, D.L., Hughes, D.C. Am J Hum Genet 2003; 73: 1271-81. • Barr, C.S., Newman, T.K., Becker, M.L., Parker, C.C., Champoux, M., Goldman, K.P., Suomi, S.J., Higley, J.D. Genes, Brain, and Behavior 2003; 2: 336-340. • Benkelfat, C. Ellenbogen, M.A., Dean, P. Arch Gen Psychiatry 1994; 51: 687-697. • Capsi, A., Sugden, K., Moffitt, T.E., Taylor, A., Craig, I.W., Harrington, H., McClay, J., Mill, J., Martin, J., Braithwaite, A., Poulton, R. Science 2003; 301: 386-389. • Cohen, C.B. Kennedy Institute of Ethics Journal 1998; 8: 111-130. • Delgado, P.L. J Clin Psychiatry 2000;suppl6: 7-11.
Works Consulted Continued • Eley, T.C., Sugden, K., Corsico, A., Gregory, A.M., Sham, P., McGuffin, P., Plomin, R., Craig, I.W. Molecular Psychiatry 2004; 9: 908-915. • Grabe, H.J., Lange, M., Wolff, B., Volzke, H., Lucht, M., Freyberger, H.J., John, U., Cascorbi, I. Molecular Psychiatry 2005; 10: 220-224. • Gibbons, R.D., Davis, J.M. Acta Psychiatr Scand 1984; 74: 8-12. • Hariri, A.R., Drabant, E.M., Munoz, K.E., Kolachana, B.S., Mattay, V.S., Egan, M.F., Weinberger, D.R. Arch Gen Psychiatry 2005; 62: 146-152. • Hirschfeld, R.M.A. J Clin Psychiatry 2000; suppl 6:4-6. • Kaufman, J., Yang, B.Z., Douglas-Palumberi, H., Houshyar, S., Lipschitz, D., Krystal, J.H., Gelernter, J. PNAS 2004 101: 17316-17321 • Lesch, K.P. J Psychiatry Neurosci 2004; 29: 174-184.
Works Consulted Continued • Lesch, K.P., Bengel, D., Heils, A., Sabol, S.Z., Greenberg, B.D., Petri, S., Benjamin, J., Muller, C.R., Hamer, D.H., Murphy, D.L. Science 1996;274: 1527-1531. • Leonard, B.E. J Clin Psychiatry 2000; suppl 6: 12-17. • Lowther, S., DePaermentier, F., Cheetham, S.C., Crompton, M.R., Katona, C.L.E., Horton, R.W. Journal of Affective Disorders 1997; 42: 199-207 • Morley, K.I., Hall, W.D., Carter, L. Australian and New Zealand Journal of Psychiatry 2004; 38: 73-80. • Stanley, M., Mann, J.J. Lancet 1983; 1: 214-216. • Tang, C.J. and Lopez, A.D. Lancet 1997; 349:1498. • Zubenko, G.S., Maher, B., Hughes, H.B. 3rd, Zubenko, W.N., Stiffler, J.S., Kaplan, B.B. Am J Med Genet 2003; 123B: 1-18